
Introduction
Invasive lobular carcinoma is the second most common histologic form of breast cancer, representing 5% to 15% of all invasive breast cancers.[1] It is composed of non-cohesive cells individually dispersed or organized in a single-file linear pattern in a fibrous stroma. Invasive lobular carcinoma is usually associated with lobular carcinoma in situ. It is now recognized as a biologically distinct disease from the more common invasive ductal carcinoma, with unique molecular pathogenesis and consequential implications on diagnosis and treatment. An understanding of these differences is crucial to tailor management strategies.[2]
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
Molecular studies have been instrumental in highlighting the role of E-cadherin inactivation in the development of lobular lesions and in supporting the notion that lobular carcinoma in situ and atypical lobular hyperplasia are, nonobligate precursors for the development of invasive cancer, rather than being simply risk indicators for invasive disease.[3]
Germline CDH1 mutations and the role of genes of the phosphatidylinositol 3-kinase pathway, PIK3CA in the development of lobular breast cancer, is considered important.[4]
Epidemiology
The incidence of breast cancer according to GLOBOCAN 2018 in the world is 46.3 per 100,000 inhabitants, while in the United States the incidence is 84.9 cases per 100,000 inhabitants, and a death rate of 12.7 deaths per 100,000 - which is the second leading cause for death among all cancers after lung cancer. Lobular carcinoma of the breast represents approximately 5% to 15% of all invasive breast cancers, with an average age at diagnosis three years greater than invasive ductal carcinoma.[5] In recent studies, they found that lobular tumors are more likely to be Luminal A between 45% to 51%, these, in turn, are less frequent in young (≤ 50 years) and Black women, and are larger, low grade, with less frequency of TP53 pathway defects and with a tendency to be diagnosed in late stages.[6]
Pathophysiology
Infiltrating lobular breast cancer has low rates (0 to 11%) of complete pathological response after neoadjuvant chemotherapy. The positive resection margins after breast conservation surgery are relatively frequent. 17% to 65% of the cases undergo another surgical intervention. The detection rates of mutations in CDH1/E-cadherin range between 12% and 83%. Several additional molecular factors, namely TP53, PIK3CA, FOXA1, ZNF703, FGFR1, and BCAR4, have been linked to infiltrating lobular breast cancer or the evolution of lobular carcinoma in situ to invasive cancer.[7][8]
Histopathology
Macroscopic Findings
Invasive lobular carcinomas frequently present as irregular and poorly delimited tumors that can be difficult to define macroscopically because of the diffuse growth pattern of the cell infiltrate. The size of the ILC is additionally difficult to work out, although it has been reported to be slightly larger than that of invasive carcinoma of no special type in some series.[9]
Microscopic Findings
Invasive lobular carcinoma is histologically characterized by a proliferation of small cells lacking cohesion and are often dispersed individually through a fibrous connective tissue or organized in single-file linear cords invading the stroma. The infiltrating cords often present a concentric pattern around normal ducts. There is usually little host reaction of the background architecture. The neoplastic cells have round or notched ovoid nuclei and a thin rim of cytoplasm with an occasional intracytoplasmic lumen, often harboring a central mucoid inclusion. Mitoses are typically infrequent.
Histological Variants
Several variants of invasive lobular carcinoma have been described that share either the cytological or growth pattern of classic invasive lobular carcinoma, but all lack cell-to-cell cohesion.
- Solid type
- Pleomorphic lobular carcinoma
- Tubulo-lobular variant
- Alveolar variant
- Mixed type
Immunoprofile
Although the literature suggests that 80% to 95% of invasive lobular carcinomas are positive for estrogen receptor (ER), in current practice, classic invasive lobular carcinomas are almost invariably ER-positive. In comparison, 70-80% of invasive carcinoma of nos special type are ER-positive. Progesterone receptor (PR) positivity is found in 60% to 70% of both tumor types.[10]
HER2 overexpression and amplification are rare in invasive lobular carcinoma, although evident in some pleomorphic lobular carcinomas.
The expression of p53, basal markers (keratin 14, keratin 5/6, EGFR) and myoepithelial markers (smooth muscle actin, and p63), is rare in invasive lobular carcinoma.[11][10]
The proliferation rate, measured by MIB1/Ki67 labeling, is generally low in invasive lobular carcinoma, although higher in the variants.[12]
One of the most consistent molecular alterations in invasive lobular carcinoma and its variants is the loss of expression of the cell-cell adhesion molecule E-cadherin, which contributes to the characteristic discohesive nature of lobular cells.[13]
Histological Grading
Histologic grading of invasive lobular carcinomas consistent with the Nottingham system is suggested, although it clearly correlates with the nuclear grade. Pure lobular tumors receive a 3 for tubule formation, only nuclear grade 1 lesion is of histologic grade 1, whereas the majority of invasive lobular carcinomas display nuclear grade 2, qualifying thus for a histologic grade 2. Because the mitotic rate is low, except for some pleomorphic invasive lobular carcinomas, few tumors are of histologic grade 3.[12]
History and Physical
Patients with invasive lobular carcinoma present with a mass or vague, diffuse nodularity. They are also detectable by mammographic breast screening. The gross pathologic and clinical features of invasive lobular carcinoma are similar to other forms of invasive breast cancer.
Invasive lobular cancer tends to stay clinically silent and escapes detection on a mammogram or physical examination until the disease is detected at advanced stages. This is secondary to the indolent growth and to the pattern of infiltrative growth of this neoplasm, which makes early diagnosis difficult with a mammogram.[14]
Patients in advanced stages have a palpable mass, sometimes with a slight thickening of the nipple or an exudative scab on the skin, other changes in the skin such as flushing, swelling, the probability of metastasis within the axillary or supraclavicular lymph nodes. Therefore, the doctor should examine the patient very well so that nothing relevant is lost.[15]
It is very important to note that patients with gastric symptoms and a medical history of mammary cancer, namely invasive lobular carcinoma, should undergo a regular check-up with upper digestive endoscopy to detect gastric metastases.[16]
Evaluation
The challenge with invasive lobular carcinomas is that they can be difficult to detect clinically and radiographically, and consequently tend to be larger at the time of diagnosis. They are often poorly circumscribed and can be missed on fine-needle aspiration and needle core biopsies due to low cellularity and the bland nature of the tumor cells.
Mammography
It is often difficult to diagnose invasive lobular carcinoma by mammography with higher false-negative rates than for other invasive cancers.[17]
The mammographic presentations of invasive lobular carcinoma include:
- A mass (up to 65% of cases) with irregular margins mostly speculated but sometimes circumscribed
- Architectural distortion and asymmetric, focal density
- Microcalcifications are uncommon (0 to 24%)
- Normal or benign mammographic findings in invasive lobular carcinoma are reported in 8 to 16% of cases.[17]
Ultrasonography
The different presentations of invasive lobular carcinoma on ultrasonography are [18]:
- A hypoechoic mass with irregular or indistinct margins and posterior acoustic shadowing (60%)
- Shadowing with no appearance of a mass (15 to 18%)
- Well-circumscribed mass lesions (9 to 13%)
- Ultrasonographically invisible (approximately 10%)
In one study, when investigating the role of ultrasound screening as an adjunct to annual mammography in detecting breast cancer in women with a history of lobular neoplasia diagnosed after BACAF or an excisional biopsy, it was found to improve sensitivity and the negative predictive value when used together. (Sensitivity: 83%, Specificity: 72%, Negative Predictive Value: 97%).[19]
Magnetic Resonance Imaging
MRI is useful in estimating the extent of invasive lobular carcinoma since it determines tumor margins, size, and multifocality more accurately than ultrasound and mammography.[20]
The preoperative magnetic resonance is more effective in the detection of contralateral breast cancer in an early stage with positive hormone receptors in older women at high risk of breast cancer.[21]
The most frequent manifestation of invasive lobular carcinoma is an enhancing solitary nodule with spiculated or ill-defined margins.
Significant correlations between histology and MRI enhancement patterns have been demonstrated. Classic invasive lobular carcinomas with tumor cells streaming along septa are visualized at MRI as enhancing septa without a dominant tumor focus.[22]
Treatment / Management
The treatment of invasive lobular carcinomas has been a topic of debate due to the potential bilaterality and multifocality that characterize these tumors. Determining the extent of invasive lobular carcinoma is very important in deciding the treatment modality. The multidisciplinary approach to the treatment includes surgery, hormonal therapy, radiation therapy, and chemotherapy.[23] It is a relatively slow-growing cancer that provides ample time to treat with the help of different modalities of management available.
Mastectomy/lumpectomy is the treatment of choice of invasive lobular carcinomas in most large series, and prophylactic contralateral mastectomy is not infrequently performed. If adequate preoperative investigations exclude extensive multifocal and contralateral disease, conservative treatment is most appropriate for invasive lobular carcinomas. The wider negative margins are not necessary in cases of invasive lobular cancer.
Surgery and radiotherapy provide locoregional control.[23] Markedly decreased amount of fibrotic reaction in the invasive lobular carcinomas makes it difficult for the panel of treating surgeons and pathologists to estimate the expansion of the disease while operating on the tumor and get tumor-free margins after mastectomy/lumpectomy. The course of surgery, regardless of histology, is determined by the TNM stage at presentation. Operable cancer may be approached with upfront surgery if amenable, or undergo surgery after preoperative neoadjuvant therapy, if appropriate.[23] Invasive lobular carcinoma can be treated similarly to invasive ductal carcinoma with surgical excision followed by radiation therapy for early-stage disease.
Adjuvant hormone therapy is also indicated, given the high percentage of cases that are positive for ER and PR.[24](B3)
Chemotherapy is of limited benefit for patients with invasive lobular carcinoma, owing to the low proliferation rates observed in the vast majority of classic invasive lobular carcinoma.[25](B3)
The factors like age, lymph nodes status, tumor size, Ki-67 biomarker, hormonal status can be associated with both recurrence and survival, and histology alone cannot be considered the only predictor.[26]
Differential Diagnosis
The differential diagnoses of invasive lobular carcinoma include both carcinomatous and non-carcinomatous neoplasms :
- Invasive ductal carcinoma with lobular features
- Gastric signet ring carcinoma metastatic to the breast
- Sclerosing epithelioid fibrosarcoma
- Leukemic and lymphomatous involvement of the breast
- Rosai-Dorfman disease
- Granular cell tumor
Surgical Oncology
Breast-conserving surgery (wide local excision) with radiotherapy or mastectomy, depending on the site and size of the tumor and patient choice, is an adequate treatment modality for invasive lobular carcinomas as for other invasive breast cancers. Nonrandomized studies reported that patient survival and local recurrence rates are similar to those of ductal/no special type carcinoma at 5 years when managed by breast-conserving surgery therapy.[27] However, late recurrences in patients who were followed up for 10 years have been reported.[28] Conversion from wide local excision to mastectomy because of positive margins after re-excision has been reported as being required more frequently in patients treated for invasive lobular carcinoma by initial breast-conserving surgery.[29] This is particularly the case for those who have been treated with neoadjuvant chemotherapy; approximately 50% of patients with invasive lobular carcinoma in some series required completion mastectomy to obtain complete excision of disease, due to incomplete resection margins after neoadjuvant therapy.[30] There is also evidence that invasive lobular carcinoma may intrinsically be less responsive to neoadjuvant chemotherapy than invasive carcinoma of ductal/no special type. Conversely, a better response to adjuvant endocrine therapy is described, with a greater improvement in survival in patients with invasive lobular carcinoma receiving hormone therapy compared with those matched patients with ductal/no special type breast cancers.[31]
Radiation Oncology
Radiation therapy following breast-conserving surgery remains the quality of care. It not only decreases the prospect of recurrence within the breast but also improves overall survival.
The substitution of hormonal therapy for radiotherapy could also be a good option in older women with a very limited life expectancy.
Standard fractionation involves extending the radiation over six to 6.5 weeks.
A boost dose of radiation to the lumpectomy site tends to decrease recurrences within the breast. The absolute benefit of the additional radiation is greater in younger women.
Treatment Planning
Although the overarching concepts of treatment are common amongst all breast cancer histological types, most surgeons favor mastectomy relating to factors specific to the patient and other pathological findings. The largely estrogen receptor-positive phenotype of invasive lobular carcinoma is central to the principles of management and the observed responses.
Medical Oncology
Leptomeningeal carcinomatosis(LC) is one of the rare but possible manifestations of the metastasis of ILC. LC commonly presents an initial symptom of headache and requires CSF cytological workup and analysis along with MRI. It is usually responsive to intra-CSF chemotherapy, radiotherapy and supportive care.[32]
Considering a fair chance to development of hypothyroidism due to radiotherapy involving or not involving the supraclavicular region, monitoring the routine thyroid function such patients regardless of treatment status is recommended taking into consideration the risk as compared to the general population.[33]
Staging
Staging of invasive lobular carcinoma of the breast is established clinically by imaging studies and physical examination before treatment and is determined pathologically based on histopathological examination of the primary tumor and regional lymph nodes after surgery.
The most commonly used clinical staging system for invasive lobular breast carcinoma is the one adopted by the American Joint Commission on Cancer (AJCC) and the International Union for Cancer Control.
Its basis is the TNM system (T, tumor; N, nodes; M, metastases). T, N, and M are compound to make five stages (stage 0, I, II, III, and IV) that reveal information about the extent of the regional neoplasm (tumor size, nodal involvement, chest-wall invasion, or skin involvement) and metastasis to distant sites.
Prognosis
Several studies have shown that invasive lobular carcinoma has the same, better, or worse prognosis than invasive ductal carcinoma. Part of this may depend on the time of follow-up and sample size because lobular carcinoma is associated with lower early local recurrence rates and a lower rate of axillary lymph node involvement at the time of diagnosis.[24][34]
Lobular carcinoma often metastasizes to the ovary, gastrointestinal tract, uterus, serosal cavities, meninges, or bone than to the regional lymph nodes or lungs.
Older age (aged > 60 years) of the patients, larger tumor size, and metastatic axillary lymph node involvement have been suggested as poor prognostic factors.[35]
Limited series reported that pleomorphic is an aggressive tumor with a frequent recurrence rate and death of patients from disease.
Complications
Axillary Nodal Metastasis
A lower frequency of axillary nodal metastasis in invasive lobular carcinoma than in invasive carcinoma of no special type has been reported in some series, the difference ranging from 3% to 10%.[36]
Distant Metastasis
Metastases of invasive lobular carcinoma differ from those of invasive carcinoma of no special type. A higher frequency of tumor extension to the bone, gastrointestinal tract, uterus, meninges, ovary, and diffuse serosal involvement is observed in invasive lobular carcinoma, while the extension to the lung is more frequent in invasive carcinoma of no special type.[37]
Postoperative and Rehabilitation Care
Breast Cancer Postoperative Care
Drain and Wound Care
Patients should receive appropriate instruction in the management of several types of wound coverage. Since surgeons often close wounds with absorbable stitches, stitch removal is not needed. We recommend that patients should shower two days after surgical intervention, including simple mastectomies and breast-conserving surgery. At the time of surgery, flexible tube drains are placed under the skin. Their role is to remove all sorts of fluids that accumulate at the site of surgery. The drain will be taken off after one to two weeks in the clinic when the drainage is minimal.
Patients should consult a doctor if there is:
- Fever (greater than or equal to 38 degrees C)
- Swelling or redness around the operation site
- Discharge around the drain site or from the wound
- Wound breakdown at the wound site
- Pain increased at the operation site
Medication and DietThe medications prescribed by doctors usually continue after surgery, and there are some diet restrictions.
Rehabilitation and Activity
Patients are encouraged to carry on normal mobility and function as early as it is possible after surgical intervention. The majority of patients with simple mastectomies and breast-conserving surgery will be able to carry on usual daily activities just after surgery, with some precautions for those with breast reconstruction.
Arm Exercise Program
The exercises promote the lymphatic system and circulation, hence preventing swelling of the concerned arm. In the first few weeks after discharge, patients should avoid over-strenuous activities.
Arm and Hand Care
Following axillary surgery, lymphedema, and increased risk of infection of the arm may occur. Hence, extra care to protect the arm and the hand on the operated side from injury is recommended. Patients usually receive a referral to a physical or occupational therapist specially-trained in treating lymphedema.
Physical Appearance
With a mastectomy, physical appearance can be maintained by undergoing breast reconstruction or wearing a prosthesis.
Consultations
- Surgical oncologist
- Oncologist
- Pharmacy oncology specialist
- Oncology nurse
- Radiation oncologist
- Medical oncologist
- Pathologist
Deterrence and Patient Education
Patients ought to be instructed to practice breast self-examination regularly and consult their doctors if they detect any abnormality.
The interprofessional team should ensure that the patients are provided with adequate information about invasive lobular carcinoma. Patients should be referred to educational websites and must be provided with written information leaflets so as to help them understand their disease, its prognosis and the different treatment modalities that are available.
Pearls and Other Issues
The survival rate of invasive lobular carcinoma of the breast is usually higher than that of invasive ductal carcinoma of the breast. Hormone replacement therapy after menopause may have some influence on the occurrence of lobular carcinoma.[38]
Enhancing Healthcare Team Outcomes
Management of invasive lobular breast carcinoma needs an interprofessional approach involving a team that consists of a surgical oncologist, a medical oncologist, a radiation oncologist, a pathologist, a radiologist, and an oncology nurse, all collaborating through disciplines to realize optimal patient results. [Level V]
After the treatment of invasive lobular breast carcinoma, long-term follow up is crucial to detect local and distant relapse. The primary care provider and NP must refer patients with any breast lump to an oncologist for further workup.
All health professionals must coordinate their actions to enhance the management of patients with invasive lobular carcinoma.
Coordination starts with excellent communication between nurses, doctors, and pharmacists. In the case of hospitalization of the patients, the prescriptions of the doctors can be discussed with the nurses, as regards the indications for the realization in practice, in a cooperative atmosphere.
Media
(Click Image to Enlarge)
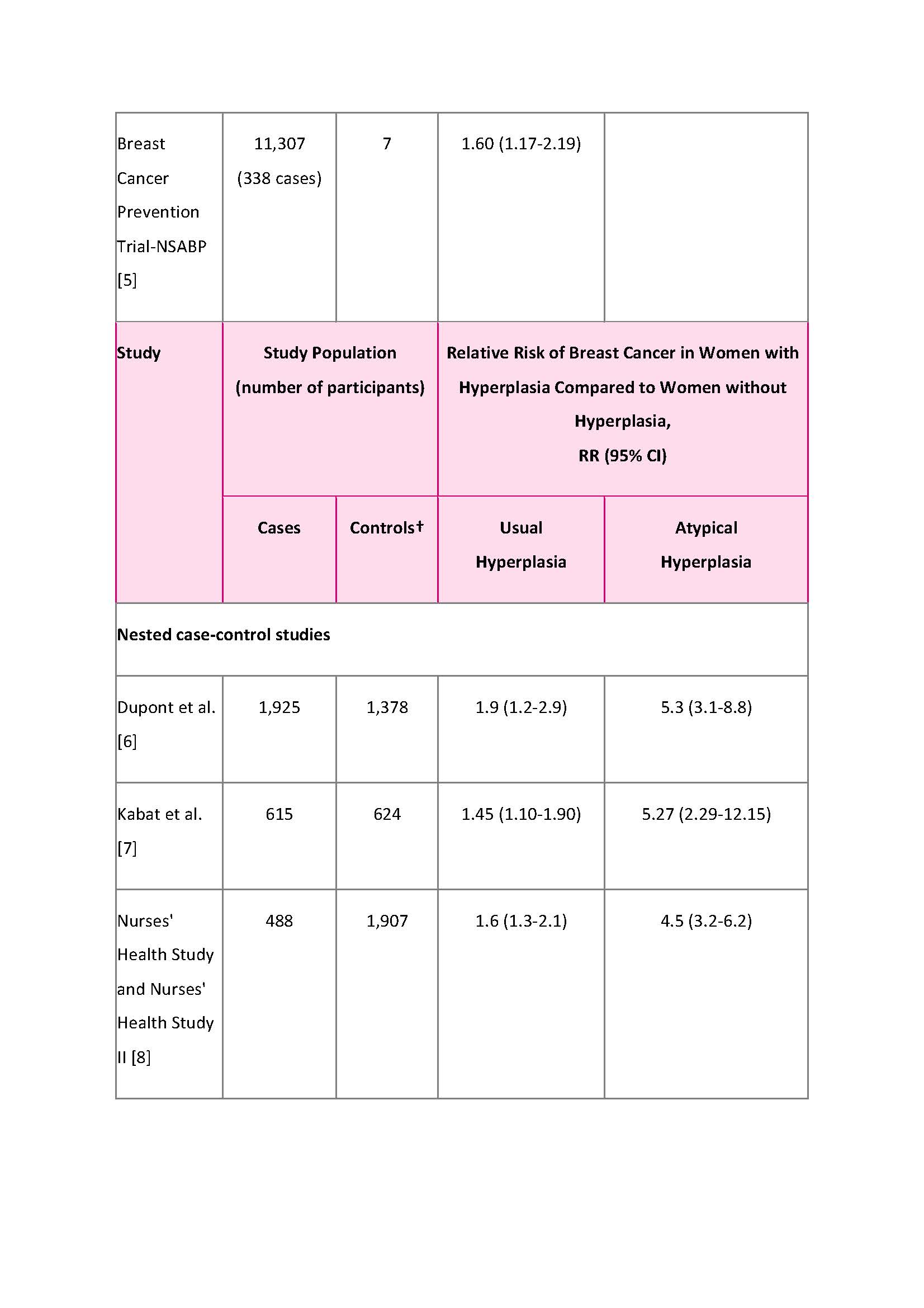
Breast Cancer Risk Factors
5. Kerlikowske K, Gard CC, Tice JA, et al. for the Breast Cancer Surveillance Consortium. Risk factors that increase risk of estrogen receptor-positive and -negative breast cancer. J Natl Cancer Inst. 109(5): djw276, 2016.
References
Rakha EA,Patel A,Powe DG,Benhasouna A,Green AR,Lambros MB,Reis-Filho JS,Ellis IO, Clinical and biological significance of E-cadherin protein expression in invasive lobular carcinoma of the breast. The American journal of surgical pathology. 2010 Oct; [PubMed PMID: 20871222]
Rakha EA,Ellis IO, Lobular breast carcinoma and its variants. Seminars in diagnostic pathology. 2010 Feb; [PubMed PMID: 20306830]
Schipper K,Seinstra D,Paulien Drenth A,van der Burg E,Ramovs V,Sonnenberg A,van Rheenen J,Nethe M,Jonkers J, Rebalancing of actomyosin contractility enables mammary tumor formation upon loss of E-cadherin. Nature communications. 2019 Aug 23 [PubMed PMID: 31444332]
Harrison BT,Nakhlis F,Dillon DA,Soong TR,Garcia EP,Schnitt SJ,King TA, Genomic profiling of pleomorphic and florid lobular carcinoma in situ reveals highly recurrent ERBB2 and ERRB3 alterations. Modern pathology : an official journal of the United States and Canadian Academy of Pathology, Inc. 2020 Jan 13 [PubMed PMID: 31932682]
McCart Reed AE,Kutasovic JR,Lakhani SR,Simpson PT, Invasive lobular carcinoma of the breast: morphology, biomarkers and 'omics. Breast cancer research : BCR. 2015 Jan 30; [PubMed PMID: 25849106]
Williams LA,Hoadley KA,Nichols HB,Geradts J,Perou CM,Love MI,Olshan AF,Troester MA, Differences in race, molecular and tumor characteristics among women diagnosed with invasive ductal and lobular breast carcinomas. Cancer causes [PubMed PMID: 30617775]
Christgen M,Steinemann D,Kühnle E,Länger F,Gluz O,Harbeck N,Kreipe H, Lobular breast cancer: Clinical, molecular and morphological characteristics. Pathology, research and practice. 2016 Jul; [PubMed PMID: 27233940]
Tabagua TT,Semiglazov VV,Bus'ko EA,Semiglazova TIu,Voroshnikov VV, [Clinical and morphological features and treatment for lobular breast cancer]. Voprosy onkologii. 2013; [PubMed PMID: 23909043]
Thomas M,Kelly ED,Abraham J,Kruse M, Invasive lobular breast cancer: A review of pathogenesis, diagnosis, management, and future directions of early stage disease. Seminars in oncology. 2019 Apr; [PubMed PMID: 31239068]
Level 3 (low-level) evidenceArpino G,Bardou VJ,Clark GM,Elledge RM, Infiltrating lobular carcinoma of the breast: tumor characteristics and clinical outcome. Breast cancer research : BCR. 2004; [PubMed PMID: 15084238]
Level 2 (mid-level) evidenceFadare O,Wang SA,Hileeto D, The expression of cytokeratin 5/6 in invasive lobular carcinoma of the breast: evidence of a basal-like subset? Human pathology. 2008 Mar; [PubMed PMID: 18261623]
Orvieto E,Maiorano E,Bottiglieri L,Maisonneuve P,Rotmensz N,Galimberti V,Luini A,Brenelli F,Gatti G,Viale G, Clinicopathologic characteristics of invasive lobular carcinoma of the breast: results of an analysis of 530 cases from a single institution. Cancer. 2008 Oct 1; [PubMed PMID: 18704988]
Level 2 (mid-level) evidenceDe Leeuw WJ,Berx G,Vos CB,Peterse JL,Van de Vijver MJ,Litvinov S,Van Roy F,Cornelisse CJ,Cleton-Jansen AM, Simultaneous loss of E-cadherin and catenins in invasive lobular breast cancer and lobular carcinoma in situ. The Journal of pathology. 1997 Dec; [PubMed PMID: 9496256]
Owen WA,Brazeal HA,Shaw HL,Lee MV,Appleton CM,Holley SO, Focal breast pain: imaging evaluation and outcomes. Clinical imaging. 2019 Feb 12; [PubMed PMID: 30825809]
Sanders MA,Brock JE,Harrison BT,Wieczorek TJ,Hong X,Guidi AJ,Dillon DA,Max L,Lester SC, Nipple-Invasive Primary Carcinomas: Clinical, Imaging, and Pathologic Features of Breast Carcinomas Originating in the Nipple. Archives of pathology [PubMed PMID: 29431468]
Ushida Y,Yoshimizu S,Horiuchi Y,Yoshio T,Ishiyama A,Hirasawa T,Tsuchida T,Fujisaki J, Clinicopathological Features of Metastatic Gastric Tumors Originating From Breast Cancer: Analysis of Eleven Cases. World journal of oncology. 2018 Aug; [PubMed PMID: 30220947]
Level 3 (low-level) evidenceKrecke KN,Gisvold JJ, Invasive lobular carcinoma of the breast: mammographic findings and extent of disease at diagnosis in 184 patients. AJR. American journal of roentgenology. 1993 Nov; [PubMed PMID: 8273634]
Level 2 (mid-level) evidenceDiCostanzo D,Rosen PP,Gareen I,Franklin S,Lesser M, Prognosis in infiltrating lobular carcinoma. An analysis of [PubMed PMID: 2153007]
Phalak KA,Milton DR,Yang WT,Bevers TB,Dogan BE, Supplemental ultrasound screening in patients with a history of lobular neoplasia. The breast journal. 2019 Mar; [PubMed PMID: 30675929]
Helvie MA,Paramagul C,Oberman HA,Adler DD, Invasive lobular carcinoma. Imaging features and clinical detection. Investigative radiology. 1993 Mar; [PubMed PMID: 8486484]
Susnik B,Schneider L,Swenson KK,Krueger J,Braatz C,Lillemoe T,Tsai M,DeFor TE,Knaack M,Rueth N, Predictive value of breast magnetic resonance imaging in detecting mammographically occult contralateral breast cancer: Can we target women more likely to have contralateral breast cancer? Journal of surgical oncology. 2018 Jul; [PubMed PMID: 30196538]
Yeh ED,Slanetz PJ,Edmister WB,Talele A,Monticciolo D,Kopans DB, Invasive lobular carcinoma: spectrum of enhancement and morphology on magnetic resonance imaging. The breast journal. 2003 Jan-Feb; [PubMed PMID: 12558665]
Mamtani A,King TA, Lobular Breast Cancer: Different Disease, Different Algorithms? Surgical oncology clinics of North America. 2018 Jan; [PubMed PMID: 29132567]
Sastre-Garau X,Jouve M,Asselain B,Vincent-Salomon A,Beuzeboc P,Dorval T,Durand JC,Fourquet A,Pouillart P, Infiltrating lobular carcinoma of the breast. Clinicopathologic analysis of 975 cases with reference to data on conservative therapy and metastatic patterns. Cancer. 1996 Jan 1; [PubMed PMID: 8630916]
Level 3 (low-level) evidenceKatz A, Does neoadjuvant/adjuvant chemotherapy change the natural history of classic invasive lobular carcinoma? Journal of clinical oncology : official journal of the American Society of Clinical Oncology. 2005 Sep 20; [PubMed PMID: 16170189]
Level 3 (low-level) evidenceDessauvagie B,Thomas A,Thomas C,Robinson C,Combrink M,Budhavaram V,Kunjuraman B,Meehan K,Sterrett G,Harvey J, Invasive lobular carcinoma of the breast: assessment of proliferative activity using automated Ki-67 immunostaining. Pathology. 2019 Dec [PubMed PMID: 31630876]
Stolier AJ,Barre G,Bolton JS,Fuhrman GM,Looney S, Breast conservation therapy for invasive lobular carcinoma: the impact of lobular carcinoma in situ in the surgical specimen on local recurrence and axillary node status. The American surgeon. 2004 Sep [PubMed PMID: 15481302]
Level 2 (mid-level) evidenceStucky CC,Gray RJ,Wasif N,Dueck AC,Pockaj BA, Increase in contralateral prophylactic mastectomy: echoes of a bygone era? Surgical trends for unilateral breast cancer. Annals of surgical oncology. 2010 Oct [PubMed PMID: 20853055]
Level 2 (mid-level) evidenceYeatman TJ,Cantor AB,Smith TJ,Smith SK,Reintgen DS,Miller MS,Ku NN,Baekey PA,Cox CE, Tumor biology of infiltrating lobular carcinoma. Implications for management. Annals of surgery. 1995 Oct [PubMed PMID: 7574934]
Cristofanilli M,Gonzalez-Angulo A,Sneige N,Kau SW,Broglio K,Theriault RL,Valero V,Buzdar AU,Kuerer H,Buchholz TA,Hortobagyi GN, Invasive lobular carcinoma classic type: response to primary chemotherapy and survival outcomes. Journal of clinical oncology : official journal of the American Society of Clinical Oncology. 2005 Jan 1 [PubMed PMID: 15625359]
Rakha EA,El-Sayed ME,Powe DG,Green AR,Habashy H,Grainge MJ,Robertson JF,Blamey R,Gee J,Nicholson RI,Lee AH,Ellis IO, Invasive lobular carcinoma of the breast: response to hormonal therapy and outcomes. European journal of cancer (Oxford, England : 1990). 2008 Jan; [PubMed PMID: 18035533]
Level 2 (mid-level) evidenceFranzoi MA,Hortobagyi GN, Leptomeningeal carcinomatosis in patients with breast cancer. Critical reviews in oncology/hematology. 2019 Mar [PubMed PMID: 30819451]
Smith GL,Smith BD,Giordano SH,Shih YC,Woodward WA,Strom EA,Perkins GH,Tereffe W,Yu TK,Buchholz TA, Risk of hypothyroidism in older breast cancer patients treated with radiation. Cancer. 2008 Mar 15 [PubMed PMID: 18213620]
Level 2 (mid-level) evidenceVandorpe T,Smeets A,Van Calster B,Van Hoorde K,Leunen K,Amant F,Moerman P,Deraedt K,Brouckaert O,Van Huffel S,Wildiers H,Christiaens MR,Neven P, Lobular and non-lobular breast cancers differ regarding axillary lymph node metastasis: a cross-sectional study on 4,292 consecutive patients. Breast cancer research and treatment. 2011 Jul; [PubMed PMID: 21562708]
Level 2 (mid-level) evidenceMersin H,Yildirim E,Gülben K,Berberoğlu U, Is invasive lobular carcinoma different from invasive ductal carcinoma? European journal of surgical oncology : the journal of the European Society of Surgical Oncology and the British Association of Surgical Oncology. 2003 May [PubMed PMID: 12711296]
Level 2 (mid-level) evidenceLamovec J,Bracko M, Metastatic pattern of infiltrating lobular carcinoma of the breast: an autopsy study. Journal of surgical oncology. 1991 Sep; [PubMed PMID: 1653879]
Shetty MR, Infiltrating lobular carcinoma: is it different from infiltrating duct carcinoma? Cancer. 1994 Aug 1; [PubMed PMID: 8039131]
Level 3 (low-level) evidenceRisk of Breast Cancer Rises with Duration of Menopausal Hormone Therapy. The American journal of nursing. 2019 Dec [PubMed PMID: 31764035]