
Introduction
Glucose is a 6-carbon structure with the chemical formula C6H12O6. Carbohydrates are ubiquitous energy sources for every organism worldwide and are essential to fuel aerobic and anaerobic cellular respiration in simple and complex molecular forms.[1] Glucose often enters the body in isometric forms such as galactose and fructose (monosaccharides), lactose and sucrose (disaccharides), or starch (polysaccharides). Excess glucose is stored in the body as glycogen, a glucose polymer, utilized during fasting. In addition, glucose can be produced through gluconeogenesis, a process involving the breakdown of fats and proteins.[2] Given the paramount importance of carbohydrates in maintaining homeostasis, numerous sources contribute to glucose production.
The sugar molecule travels through the blood to energy-requiring tissues when glucose is in the body.[3] Glucose undergoes a series of biochemical reactions, releasing energy as adenosine triphosphate (ATP). ATP derived from these processes fuels virtually every energy-requiring process in the body. In eukaryotes, most energy derives from aerobic (oxygen-requiring) processes, which start with a glucose molecule. Glucose is initially broken down through the anaerobic process of glycolysis, producing some ATP and pyruvate as end products. Under anaerobic conditions, pyruvate converts to lactate through reduction.[4] Conversely, under aerobic conditions, the pyruvate can enter the citric acid cycle to generate energy-rich electron carriers that produce ATP at the electron transport chain.[5]
Cellular Level
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Cellular Level
Glucose reserves are stored as the polymer glycogen in humans. Glycogen is present in the highest concentrations in the liver and muscle tissues. The regulation of glycogen, and thus glucose, is primarily controlled by the peptide hormones insulin and glucagon. These hormones are produced in the pancreatic islet of Langerhans—glucagon from α-cells and insulin from β-cells. The balance between these 2 hormones depends on the body's metabolic state, whether fasting or energy-rich, with insulin in higher concentrations during energy-rich states and glucagon during fasting. Through signaling cascades regulated by these hormones, glycogen is either catabolized, liberating glucose promoted by glucagon during fasting, or synthesized, further consuming excess glucose facilitated by insulin during times of energy abundance. Insulin and glucagon, among other hormones, also control glucose transport in and out of cells by altering the expression of glucose transporter type 4 (GLUT-4).[6][7]
Glucose Transporters
Several glucose transporters are in the human body, with differential expression varying by tissue type. These transporters are differentiated into 2 main categories—sodium-dependent transporters (SGLTs) and sodium-independent transporters (GLUT). The SGLTs rely on the active transport of sodium across the cell membrane, which then diffuses down the concentration gradient along with a glucose molecule, known as secondary active transport. The sodium-independent transporters do not rely on sodium and transport glucose using facilitated diffusion. Of the sodium-independent transporters, only GLUT4's expression is affected by insulin and glucagon. The most important classes of glucose transporters and their characteristics are listed below (see Image. Glucose Transporters).
- SGLT: Found primarily in the renal tubules and intestinal epithelia, SGLTs are essential for glucose reabsorption and absorption. This transporter works through secondary active transport as it requires ATP to actively pump sodium out of the cell and into the interstitial space through sodium/potassium exchange to establish a favorable concentration gradient for the SGLT. The SGLT between the renal tubule lumen and the intracellular space uses the passive transport of sodium into the cell to drive the cotransport of glucose into the cell.
- GLUT-1: Found primarily in the pancreatic β-cells, red blood cells, and hepatocytes. This bi-directional transporter is essential for glucose sensing by the pancreas, an important aspect of the feedback mechanism in controlling blood glucose with endogenous insulin.
- GLUT-2: Found primarily in hepatocytes, pancreatic β-cells, intestinal epithelium, and renal tubular cells. This bi-directional transporter is essential for regulating glucose metabolism in the liver.
- GLUT-3: This transporter is found primarily in the central nervous system and has a high affinity for glucose, consistent with the brain's increased metabolic demands.
- GLUT-4: Found primarily in skeletal muscle, cardiac muscle, adipose tissue, and brain tissue. This transporter gets stored in cytoplasmic vesicles in an inactive state, which merges with the cell membrane when stimulated by insulin. These transporters undergo a 10- to 20-fold increase in density during times of energy abundance upon insulin release with the net effect of a decrease in blood glucose. Glucose more readily enters the cells that have GLUT-4 on their surface.[8][9][10][11]
Central Role of Glucose in Carbohydrate Metabolism
The end products of carbohydrate digestion in the alimentary tract are predominantly glucose, fructose, and galactose, with glucose comprising 80% of the end product. After absorption from the alimentary canal, a significant portion of the fructose and almost all of the galactose rapidly convert into glucose in the liver. Therefore, only a small quantity of fructose and galactose is present in the blood. Thus, glucose is the final common pathway for transporting all carbohydrates to the tissue cells.
In liver cells, appropriate enzymes are available to promote interconversions among the monosaccharides glucose, fructose, and galactose. The dynamics of the enzymes are such that when the liver releases the monosaccharides, the final product is always glucose. The reason is that the hepatocytes contain a large amount of glucose phosphatase. Glucose-6-phosphate can be broken down into glucose and phosphate, and glucose is transported through the liver cell membrane and back into the blood.[12]
Organ Systems Involved
Glucose is essential for the proper functioning of every organ system. However, specific organs are particularly crucial in regulating its levels.
Liver
The liver plays a crucial role in regulating blood glucose levels. Glycogen, a multibranched polysaccharide of glucose, is the storage form of glucose in the human body, primarily found in the liver and skeletal muscle. Glycogen functions as the body's short-term storage of glucose, whereas triglycerides in adipose tissues serve as the long-term storage. Glucose is released from glycogen when stimulated by glucagon and during fasting conditions, thereby increasing blood glucose levels. Glucose is added to glycogen under the control of insulin and energy-rich conditions, lowering blood glucose levels.[13]
Pancreas
The pancreas releases the hormones that are primarily responsible for controlling blood glucose levels. When glucose concentration rises within the β-cells, insulin is released, leading to a decrease in blood glucose through various mechanisms outlined below. Conversely, when glucose levels drop and insulin levels decrease (directly influenced by low glucose levels), α-cells of the pancreas release glucagon, which raises blood glucose through several mechanisms. In addition, somatostatin is released from γ-cells of the pancreas and has a net effect of decreasing blood glucose levels.[14][15][16]
Adrenal Gland
The adrenal gland consists of the cortex and the medulla, which play roles in glucose homeostasis. The adrenal cortex releases glucocorticoids, notably cortisol, which raise blood glucose levels through the mechanisms described below. The adrenal medulla releases epinephrine, increasing blood glucose levels through the following mechanisms.[17]
Thyroid Gland
The thyroid gland is responsible for the production and release of thyroxine. Thyroxine affects nearly all tissues in the body, including raising blood glucose levels.[18]
Anterior Pituitary Gland
The anterior pituitary gland releases adrenocorticotropic and growth hormones, increasing blood glucose levels.[19]
Hormones
Many hormones are involved in glucose homeostasis. Understanding each hormone's mechanism and net effect is essential. Remembering which ones lower glucose levels, primarily insulin and somatostatin, can help understand their functions. The other hormones increase glucose levels.
- Insulin: Decreases blood glucose levels through increased expression of GLUT4, increased expression of glycogen synthase, inactivation of phosphorylase kinase (thus decreasing gluconeogenesis), and decreased expression of rate-limiting enzymes involved in gluconeogenesis.
- Glucagon: Increases blood glucose levels through increased glycogenolysis and gluconeogenesis.
- Somatostatin: Decreases blood glucose levels through local suppression of glucagon release and suppression of gastrin and pituitary tropic hormones. This hormone also decreases insulin release; however, the net effect is decreased blood glucose levels.
- Cortisol: Increases blood glucose levels through the stimulation of gluconeogenesis and the antagonism of insulin.
- Epinephrine: Increases blood glucose levels through glycogenolysis (glucose release from glycogen) and increased fatty acid release from adipose tissues, which can be catabolized and enter gluconeogenesis.
- Thyroxine: Increases blood glucose levels through glycogenolysis and increased absorption in the intestine.
- Growth hormone: Promotes gluconeogenesis, inhibits liver uptake of glucose, stimulates thyroid hormone, and inhibits insulin.
- Adrenocorticotropic hormone: Stimulates cortisol release from adrenal glands and promotes the release of fatty acids from adipose tissue, contributing to gluconeogenesis.[20]
Related Testing
Fasting Blood Glucose Test
This test is standard to measure glucose levels in the bloodstream after an overnight fast of at least 8 hours. The sample is typically collected before breakfast to ensure fasting conditions. Blood glucose levels are assessed using enzymatic assays or automated laboratory analyzers to determine glucose concentration in the plasma or serum. Normal fasting blood glucose levels typically range from 70 to 100 mg/dL (3.9 to 5.6 mmol/L).[21]
Random Blood Glucose Testing
This test is a valuable diagnostic tool for assessing blood glucose levels without fasting or preplanning. The sample is analyzed using a glucometer or laboratory assay to determine the glucose concentration in the bloodstream. Unlike fasting glucose tests or oral glucose tolerance tests, the test provides an immediate snapshot of blood glucose levels, facilitating rapid clinical decision-making. In patients without diabetes mellitus, normal glucose levels typically range from 70 to 140 mg/dL (3.9 to 7.8 mmol/L).[22] These values may vary slightly depending on the laboratory reference range and patient-specific factors.[23]
Oral Glucose Tolerance Test
This test is valuable in assessing glucose metabolism, offering insights into the body's response to ingested glucose. The test aids in the early detection of diabetes and pre-diabetes mellitus, enabling timely interventions to prevent or delay disease progression and associated complications. The test involves administering a standardized oral glucose load, typically 75 g, after an overnight fast, followed by serial blood glucose measurements at specified intervals, typically 0, 30, 60, 90, and 120 minutes post-glucose ingestion. Blood samples are collected to assess glucose concentrations, reflecting the body's ability to handle a glucose challenge.[24][25]
Normal response: In individuals with normal glucose tolerance, blood glucose levels rise temporarily following glucose ingestion but return to fasting levels within 2 hours. Normal oral glucose tolerance test results indicate efficient glucose uptake and insulin secretion, indicative of intact glucose metabolism.
Impaired glucose tolerance: Impaired glucose tolerance is characterized by elevated blood glucose levels during the oral glucose tolerance test, exceeding normal thresholds but not meeting the diagnostic criteria for diabetes mellitus. This condition represents an intermediate stage of dysglycemia, placing individuals at risk of developing diabetes mellitus and cardiovascular complications.
Diabetes mellitus is diagnosed when the oral glucose tolerance test reveals sustained hyperglycemia, with fasting glucose ≥126 mg/dL (7.0 mmol/L) or 2-hour post-load glucose levels ≥200 mg/dL (11.1 mmol/L) on 2 separate occasions. The oral glucose tolerance test is particularly useful for diagnosing gestational diabetes mellitus, a transient form of diabetes mellitus occurring during pregnancy.[26]
Pathophysiology
Glucose metabolism is intricately regulated to meet cell energy demands while preventing hyperglycemia or hypoglycemia. The dysregulation of glucose homeostasis underlies the pathogenesis of several metabolic disorders, posing significant health challenges worldwide. Understanding the pathophysiology of glucose dysregulation provides insights into the molecular mechanisms driving metabolic disorders.[27]
- Type 1 diabetes: Type 1 diabetes results from autoimmune destruction of pancreatic β-cells, leading to insulin deficiency. Insulin secretion loss impairs peripheral tissue glucose uptake, resulting in hyperglycemia and metabolic derangements.
- Type 2 diabetes: Type 2 diabetes primarily arises from insulin resistance, characterized by diminished cellular response to insulin. Peripheral tissues fail to efficiently utilize glucose, leading to compensatory hyperinsulinemia, β-cell exhaustion, and eventual pancreatic dysfunction.
- Reactive hypoglycemia: Reactive hypoglycemia occurs postprandially due to excessive insulin secretion in response to carbohydrate-rich meals. This exaggerated insulin release leads to rapid glucose clearance, resulting in hypoglycemic episodes.
- Fasting hypoglycemia: Fasting hypoglycemia can stem from various etiologies, including hormonal deficiencies, liver disease, or metabolic enzyme deficiencies, disrupting the balance between glucose production and utilization during fasting periods.
- Metabolic syndrome: Metabolic syndrome encompasses a cluster of metabolic abnormalities, including central obesity, insulin resistance, dyslipidemia, and hypertension, predisposing individuals to cardiovascular disease and type 2 diabetes. Insulin resistance plays a central role in the pathogenesis of metabolic syndrome, driving aberrant glucose and lipid metabolism.[28][29][30]
Clinical Significance
The pathology associated with glucose often occurs when blood glucose levels are too high or too low. The following summarizes some of the more common pathological states linked to alterations in glucose levels and the associated pathophysiology.
Hyperglycemia
Hyperglycemia can induce pathology, both acutely and chronically. Type 1 and 2 diabetes are both disease states characterized by chronically elevated blood glucose levels that, over time and with poor glucose control, lead to significant morbidity.[31] Both types of diabetes have multifocal etiologies—type 1 is associated with genetic, environmental, and immunological factors and most often presents in pediatric patients, whereas type 2 is associated with comorbid conditions such as obesity in addition to genetic factors and is more likely to manifest in adulthood. Type 1 diabetes results from the autoimmune destruction of pancreatic β-cells and insulin deficiency, whereas type 2 diabetes results from peripheral insulin resistance due to metabolic dysfunction, often in the setting of obesity. In both cases, the result is inappropriately elevated blood glucose levels, which can lead to pathology through various mechanisms.
- Osmotic damage: Glucose is osmotically active and can cause damage to peripheral nerves.
- Oxidative stress: Glucose participates in several reactions that produce oxidative byproducts.
- Non-enzymatic glycation: Glucose can form complexes with lysine residues on proteins, leading to structural and functional disruption.[32][6]
These mechanisms lead to various clinical manifestations through both microvascular and macrovascular complications. Some include peripheral neuropathies, poor wound healing or chronic wounds, retinopathy, coronary artery disease, cerebral vascular disease, and chronic kidney disease. Understanding the mechanisms behind the pathology caused by elevated glucose levels is imperative.[33][34]
High blood sugar levels can also lead to acute pathology, most often observed in patients with type 2 diabetes, known as a hyperosmolar hyperglycemic state. This state occurs when severely elevated blood glucose levels increase plasma osmolality. The high osmolarity leads to osmotic diuresis (excessive urination) and dehydration. A variety of clinical manifestations emerge, including altered mental status, motor abnormalities, focal and global central nervous system dysfunction, nausea, vomiting, abdominal pain, and orthostatic hypotension.[35]
Hypoglycemia
Hypoglycemia is most commonly observed iatrogenically in patients with diabetes mellitus secondary to glucose-lowering drugs. This condition occurs, especially in the inpatient setting, with the interruption of the patient's usual diet. The symptoms are non-specific, but clinical findings such as relation to fasting or exercise and symptom improvement with glucose administration make hypoglycemia more likely.[36] Hypoglycemia symptoms can be described as either neuroglycopenic, due to a direct effect on the central nervous system, or neurogenic, due to sympatho-adrenergic involvement.[37] Neurogenic symptoms can be further broken down into either cholinergic or adrenergic. The following are some common symptoms of hypoglycemia.
- Neuroglycopenic: Fatigue, behavioral changes, seizures, coma, and death.
- Neurogenic: Adrenergic such as anxiety, tremor, and palpitations.
- Neurogenic: Cholinergic such as paresthesias, diaphoresis, and hunger.[38]
Taking into account what we have learned about glucose in a brief overview of glucose metabolism, let us consider the sequence of events following a carbohydrate-dense meal. Various glucose polymers are broken down in saliva and intestines, releasing free glucose. This glucose is absorbed into the intestinal epithelium through SGLT receptors apically and then enters the bloodstream through GLUT receptors on the basolateral wall. The blood glucose levels spike, triggering an increased glucose concentration in the pancreas and prompting the release of pre-formed insulin. Insulin has several downstream effects, including increased expression of enzymes involved in glycogen synthesis, such as glycogen synthase in the liver. The glucose enters hepatocytes and is added to glycogen chains. Insulin also stimulates the release of GLUT-4 from their intracellular confinement, increasing basal glucose uptake into muscle and adipose tissue as blood glucose levels dwindle. Insulin levels decrease to the low-normal range. As the insulin levels drop below the normal range, glucagon from pancreatic α-cells is released, promoting a rise in blood glucose levels through glycogenolysis and gluconeogenesis. Typically, this increases glucose levels enough to last until the next meal. However, if the patient continues to fast, the adrenomedullary system secretes cortisol and epinephrine, establishing euglycemia from a hypoglycemic state.[14][39][40]
Media
(Click Image to Enlarge)
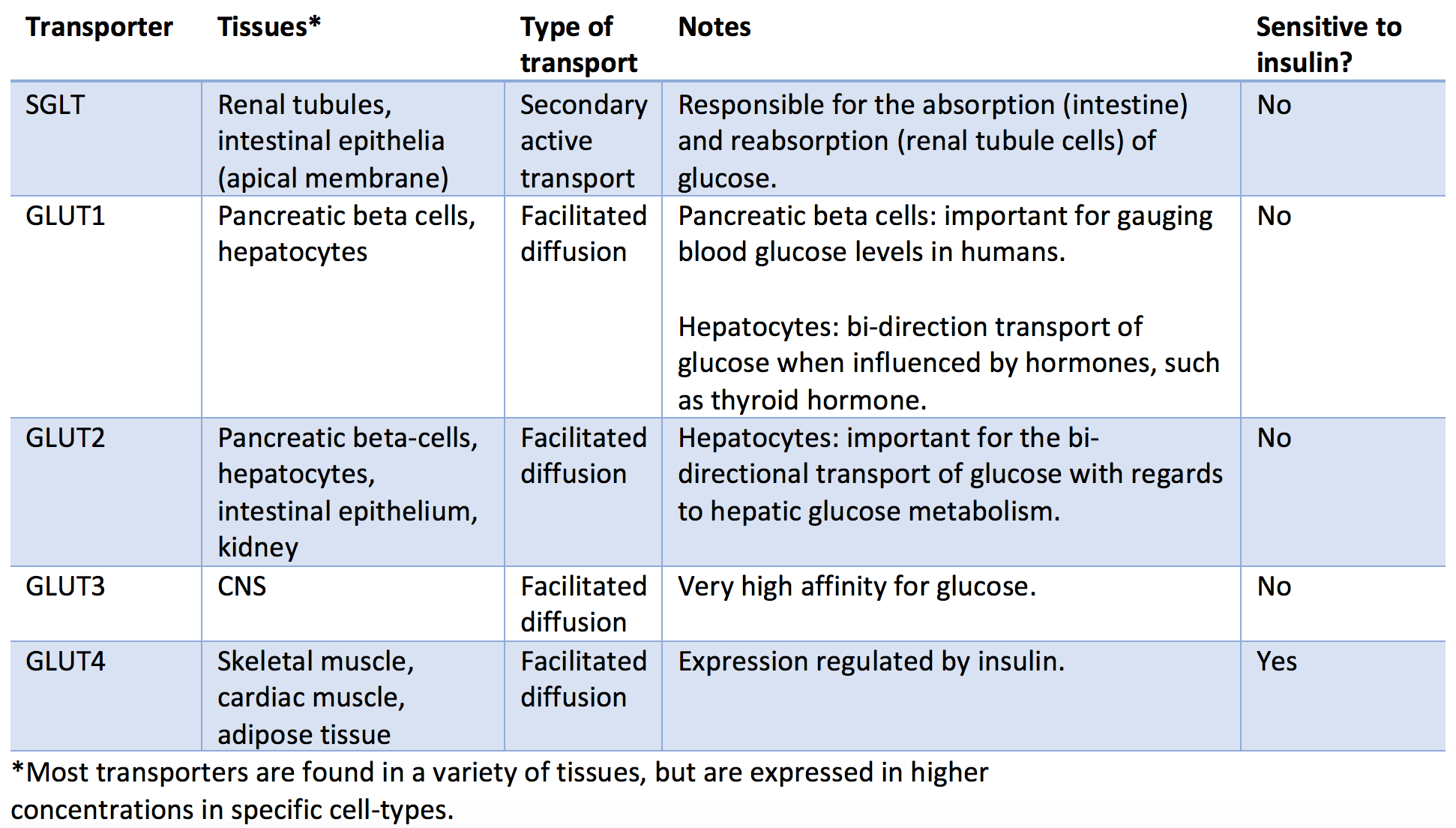
Glucose Transporters. The image depicts various classes of glucose transporters and their characteristics.
Contributed by P Hantzidiamantis
References
Yu EY, Ren Z, Mehrkanoon S, Stehouwer CDA, van Greevenbroek MMJ, Eussen SJPM, Zeegers MP, Wesselius A. Plasma metabolomic profiling of dietary patterns associated with glucose metabolism status: The Maastricht Study. BMC medicine. 2022 Nov 21:20(1):450. doi: 10.1186/s12916-022-02653-1. Epub 2022 Nov 21 [PubMed PMID: 36414942]
Remesar X, Alemany M. Dietary Energy Partition: The Central Role of Glucose. International journal of molecular sciences. 2020 Oct 19:21(20):. doi: 10.3390/ijms21207729. Epub 2020 Oct 19 [PubMed PMID: 33086579]
Goyal MS, Raichle ME. Glucose Requirements of the Developing Human Brain. Journal of pediatric gastroenterology and nutrition. 2018 Jun:66 Suppl 3(Suppl 3):S46-S49. doi: 10.1097/MPG.0000000000001875. Epub [PubMed PMID: 29762377]
Hui S, Ghergurovich JM, Morscher RJ, Jang C, Teng X, Lu W, Esparza LA, Reya T, Le Zhan, Yanxiang Guo J, White E, Rabinowitz JD. Glucose feeds the TCA cycle via circulating lactate. Nature. 2017 Nov 2:551(7678):115-118. doi: 10.1038/nature24057. Epub 2017 Oct 18 [PubMed PMID: 29045397]
Liu S, Dai Z, Cooper DE, Kirsch DG, Locasale JW. Quantitative Analysis of the Physiological Contributions of Glucose to the TCA Cycle. Cell metabolism. 2020 Oct 6:32(4):619-628.e21. doi: 10.1016/j.cmet.2020.09.005. Epub 2020 Sep 21 [PubMed PMID: 32961109]
Gurung P, Zubair M, Jialal I. Plasma Glucose. StatPearls. 2024 Jan:(): [PubMed PMID: 31082125]
Daghlas SA, Mohiuddin SS. Biochemistry, Glycogen. StatPearls. 2024 Jan:(): [PubMed PMID: 30969624]
Kellett GL, Brot-Laroche E, Mace OJ, Leturque A. Sugar absorption in the intestine: the role of GLUT2. Annual review of nutrition. 2008:28():35-54. doi: 10.1146/annurev.nutr.28.061807.155518. Epub [PubMed PMID: 18393659]
Fazakerley DJ, Koumanov F, Holman GD. GLUT4 On the move. The Biochemical journal. 2022 Feb 11:479(3):445-462. doi: 10.1042/BCJ20210073. Epub [PubMed PMID: 35147164]
Holesh JE, Aslam S, Martin A. Physiology, Carbohydrates. StatPearls. 2024 Jan:(): [PubMed PMID: 29083823]
Navale AM, Paranjape AN. Glucose transporters: physiological and pathological roles. Biophysical reviews. 2016 Mar:8(1):5-9. doi: 10.1007/s12551-015-0186-2. Epub 2016 Jan 19 [PubMed PMID: 28510148]
Srichaikul K, Jenkins DJA. The Glycemic Index, Rate of Digestion of Carbohydrate Foods, and Their Potential Link with Cardiovascular Disease. The Journal of nutrition. 2022 Apr 1:152(4):920-921. doi: 10.1093/jn/nxab427. Epub [PubMed PMID: 35174392]
Jones JG. Hepatic glucose and lipid metabolism. Diabetologia. 2016 Jun:59(6):1098-103. doi: 10.1007/s00125-016-3940-5. Epub 2016 Apr 5 [PubMed PMID: 27048250]
El Sayed SA, Mukherjee S. Physiology, Pancreas. StatPearls. 2024 Jan:(): [PubMed PMID: 29083590]
Vargas E, Joy NV, Carrillo Sepulveda MA. Biochemistry, Insulin Metabolic Effects. StatPearls. 2024 Jan:(): [PubMed PMID: 30252239]
Venugopal SK, Sankar P, Jialal I. Physiology, Glucagon. StatPearls. 2024 Jan:(): [PubMed PMID: 30725767]
Dutt M, Wehrle CJ, Jialal I. Physiology, Adrenal Gland. StatPearls. 2024 Jan:(): [PubMed PMID: 30725945]
Pirahanchi Y, Tariq MA, Jialal I. Physiology, Thyroid. StatPearls. 2024 Jan:(): [PubMed PMID: 30137850]
Rawindraraj AD, Basit H, Jialal I. Physiology, Anterior Pituitary. StatPearls. 2024 Jan:(): [PubMed PMID: 29763073]
Christensen MB. Glucose-dependent insulinotropic polypeptide: effects on insulin and glucagon secretion in humans. Danish medical journal. 2016 Apr:63(4):. pii: B5230. Epub [PubMed PMID: 27034187]
Kubihal S, Goyal A, Gupta Y, Khadgawat R. Glucose measurement in body fluids: A ready reckoner for clinicians. Diabetes & metabolic syndrome. 2021 Jan-Feb:15(1):45-53. doi: 10.1016/j.dsx.2020.11.021. Epub 2020 Dec 3 [PubMed PMID: 33310176]
Murray-Bachmann R, Leung TM, Myers AK, Murthi S, Sarbanes M, Ziskovich K, Lesser M, Poretsky L. Reliability of continuous glucose monitoring system in the inpatient setting. Journal of clinical & translational endocrinology. 2021 Sep:25():100262. doi: 10.1016/j.jcte.2021.100262. Epub 2021 Jul 7 [PubMed PMID: 34336598]
Sung JF, Taslimi MM, Faig JC. Continuous glucose monitoring in pregnancy: new frontiers in clinical applications and research. Journal of diabetes science and technology. 2012 Nov 1:6(6):1478-85 [PubMed PMID: 23294795]
Chen ME, Aguirre RS, Hannon TS. Methods for Measuring Risk for Type 2 Diabetes in Youth: the Oral Glucose Tolerance Test (OGTT). Current diabetes reports. 2018 Jun 16:18(8):51. doi: 10.1007/s11892-018-1023-3. Epub 2018 Jun 16 [PubMed PMID: 29909550]
Galant AL, Kaufman RC, Wilson JD. Glucose: Detection and analysis. Food chemistry. 2015 Dec 1:188():149-60. doi: 10.1016/j.foodchem.2015.04.071. Epub 2015 Apr 23 [PubMed PMID: 26041177]
Khan RMM, Chua ZJY, Tan JC, Yang Y, Liao Z, Zhao Y. From Pre-Diabetes to Diabetes: Diagnosis, Treatments and Translational Research. Medicina (Kaunas, Lithuania). 2019 Aug 29:55(9):. doi: 10.3390/medicina55090546. Epub 2019 Aug 29 [PubMed PMID: 31470636]
Tonelli J, Kishore P, Lee DE, Hawkins M. The regulation of glucose effectiveness: how glucose modulates its own production. Current opinion in clinical nutrition and metabolic care. 2005 Jul:8(4):450-6 [PubMed PMID: 15930973]
Level 3 (low-level) evidenceKishimoto I. Subclinical Reactive Hypoglycemia with Low Glucose Effectiveness-Why We Cannot Stop Snacking despite Gaining Weight. Metabolites. 2023 Jun 15:13(6):. doi: 10.3390/metabo13060754. Epub 2023 Jun 15 [PubMed PMID: 37367911]
Karakas SE. Reactive Hypoglycemia: A Trigger for Nutrient-Induced Endocrine and Metabolic Responses in Polycystic Ovary Syndrome. Journal of clinical medicine. 2023 Nov 23:12(23):. doi: 10.3390/jcm12237252. Epub 2023 Nov 23 [PubMed PMID: 38068304]
Chao HW, Chao SW, Lin H, Ku HC, Cheng CF. Homeostasis of Glucose and Lipid in Non-Alcoholic Fatty Liver Disease. International journal of molecular sciences. 2019 Jan 13:20(2):. doi: 10.3390/ijms20020298. Epub 2019 Jan 13 [PubMed PMID: 30642126]
Harreiter J, Roden M. [Diabetes mellitus: definition, classification, diagnosis, screening and prevention (Update 2023)]. Wiener klinische Wochenschrift. 2023 Jan:135(Suppl 1):7-17. doi: 10.1007/s00508-022-02122-y. Epub 2023 Apr 20 [PubMed PMID: 37101021]
Nawale RB, Mourya VK, Bhise SB. Non-enzymatic glycation of proteins: a cause for complications in diabetes. Indian journal of biochemistry & biophysics. 2006 Dec:43(6):337-44 [PubMed PMID: 17285797]
Level 3 (low-level) evidenceGoyal R, Singhal M, Jialal I. Type 2 Diabetes. StatPearls. 2024 Jan:(): [PubMed PMID: 30020625]
Goyal R, Nguyen M, Jialal I. Glucose Intolerance. StatPearls. 2024 Jan:(): [PubMed PMID: 29763085]
Adeyinka A, Kondamudi NP. Hyperosmolar Hyperglycemic Syndrome. StatPearls. 2024 Jan:(): [PubMed PMID: 29489232]
Awosika A, Adabanya U, Millis RM, Omole AE, Moon JH. Postprandial Hypotension: An Underreported Silent Killer in the Aged. Cureus. 2023 Feb:15(2):e35411. doi: 10.7759/cureus.35411. Epub 2023 Feb 24 [PubMed PMID: 36851946]
Morgan RK, Cortes Y, Murphy L. Pathophysiology and aetiology of hypoglycaemic crises. The Journal of small animal practice. 2018 Nov:59(11):659-669. doi: 10.1111/jsap.12911. Epub 2018 Aug 13 [PubMed PMID: 30102417]
Level 3 (low-level) evidenceMathew P, Thoppil D. Hypoglycemia. StatPearls. 2024 Jan:(): [PubMed PMID: 30521262]
Kalra A, Yetiskul E, Wehrle CJ, Tuma F. Physiology, Liver. StatPearls. 2024 Jan:(): [PubMed PMID: 30571059]
International Hypoglycaemia Study Group. Hypoglycaemia, cardiovascular disease, and mortality in diabetes: epidemiology, pathogenesis, and management. The lancet. Diabetes & endocrinology. 2019 May:7(5):385-396. doi: 10.1016/S2213-8587(18)30315-2. Epub 2019 Mar 27 [PubMed PMID: 30926258]