
Introduction
The diaphragm in the thorax is called the thoracic diaphragm and serves as an important anatomical landmark that separates the thorax, or chest, from the abdomen. It functions during breathing when it contracts to enlarge the thoracic cavity and reduce the intrathoracic pressure so that lungs may expand and fill their alveoli with air. It is a dome-shaped muscle and tendon that functions as the main muscle of respiration and is essential to the breathing process. It is a fibromuscular sheet that has a convex upper surface that forms the floor of the thoracic cavity and a concave under surface to form the roof of the abdominal cavity. The esophagus, phrenic, and vagus nerves, descending aorta, and inferior vena cava pass through the diaphragm between the thoracic and abdominal cavities. The diaphragm is asymmetric with the left side slightly more inferior than the right, chiefly because of the presence of the liver located on the right. The left side may also be partially inferiorly located because of the push by the heart.[1],[2]
Structure and Function
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Structure and Function
Functions of the Diaphragm
Muscle of Inspiration
The diaphragm pulls its central tendon down during contraction and then increases the vertical diameter of the thorax. This increases the negative pressure inside the thoracic cavity, which draws in air. Thus, the diaphragm is the most important muscle used in inspiration. During inhalation, the diaphragm contracts and is pushed inferiorly into the abdominal cavity where it appears flat. Simultaneously the external intercostal muscles located in between the ribs raise the anterior chest wall like the handles of a bucket. This results in the chest cavity becoming larger and wider, which allows air in from the outside. During exhalation, the rib cage and chest wall start to sag and revert to the original position. At the same time, there is relaxation and elevation of the diaphragm. This motion forces the air within the lungs to push out of the body.[2],[3]
Muscle of Abdominal Straining
The contraction of the diaphragm will assist in the contraction of the muscles of the anterior abdominal wall in raising the intra-abdominal pressure will normal processes like micturition, defecation, and parturition.
Weightlifting Muscle
When a person takes and holds a deep breath, the diaphragm will assist the muscles of the anterior abdominal wall to raise the intra-abdominal pressure. This maneuver is also called as Valsalva maneuver and is used to augment heart murmurs and classify them whether they are clinically right-sided or left-sided.
Thoracoabdominal Pump
When people breathe in, the diaphragm descends, which decreases the intrathoracic pressure and improves the intra-abdominal pressure. This compresses the blood in the inferior vena cava (IVC) and forces it upward into the right atrium and helps to fill the heart. When abdominal lymph vessels are also compressed, its passage upward within the thoracic duct is aided by the negative intrathoracic pressure. Furthermore, valves in the thoracic duct prevent the backflow of the lymph in the thoracic duct.
Embryology
Diaphragm Formation
- Septum transversum
- Pleuro-peritoneal membrane
- Mesentery of esophagus
- Mesoderm of the body wall
Insertion
The diaphragm inserts into a central tendon. The top surface of the tendon is partially connected to the lower surface of the fibrous pericardium. Muscle fibers arising from the right crus traverse up on the left side and encircle the orifice of the esophagus in a sling-like loop. These fibers act as a sphincter and likely assist in preventing the regurgitation of the stomach contents into the thoracic part of the esophagus.[4]
Origin of Diaphragm
Sternal
The sternal part originates as 2 fleshy slips from the back of the xiphoid process.
Costal
The costal part originates from inner surfaces of the cartilages, adjacent parts of the lower sixth ribs on each side. It interdigitates with transversus abdominis.
Lumbar
The medial lumbocostal arch is a tendinous arch in fascia covering psoas major. Medially, it attaches to the side of the body of vertebra L1. Laterally, it connects to the front of the transverse process of vertebra L1.
The lateral lumbocostal arch is a tendinous arch in fascia covering the upper part of quadratus lumborum. Medially, attach to the front of the transverse process of vertebra L1. Laterally, it connects to the lower border of the 12th rib.
The right crus arises from the anterolateral surface of the bodies of the upper three lumbar vertebrae and also the intervening intervertebral disc
The left crus arises from the corresponding parts of the upper 2 lumbar vertebrae.
Medial margin of two crura forms a tendinous arc across the front of the aorta called the median arcuate ligament.
Blood Supply and Lymphatics
Major Arteries Supplying the Diaphragm
- Musculophrenic artery branch of the internal thoracic artery
- Superior phrenic artery branch of the aorta
- Lower five intercostal arteries and subcostal artery
- Inferior phrenic artery
Nerves
Motor Nerve Supply
Right and left phrenic nerves (C3 through C5)
Sensory Nerve Supply
The phrenic nerve innervates the parietal pleura and peritoneum covering the central surfaces of the diaphragm. The lower 6 intercostal nerves supply the periphery of the diaphragm.
When the diaphragm contracts, the large-sized myelinated phrenic afferents fire. On the other hand, the smaller diameter nerves continue to discharge throughout the respiratory cycle. It is now well established that activation of both non-myelinated and myelinated phrenic sensory nerves modulate respiratory output during each breathing cycle. However, the activation of the phrenic afferents does increase significantly as the diaphragm continues to work and develops fatigue. Once the phrenic afferents are activated, they also modulate the sympathetic motor outflow. Furthermore, the phrenic afferents also contribute to somatosensation of the diaphragm and make one aware of the sensation of breathing while awake. The exact influence of the spinal and supraspinal nerves and synapses between the non-myelinated and myelinated phrenic nerves is not known.
The use of deep muscle training contributed to a significant change in the position of the body in the sagittal plane and the increase in the amplitude of breathing.[5]
Muscles
One can find the origins of the diaphragm along the lumbar vertebrae of the spine and the inferior border of the ribs and sternum.
The superior diaphragm origin is continuous from the xiphoid process anteriorly to lower 6 costal cartilages of the thorax laterally and first 2 lumbar vertebrae posteriorly. The musculoskeletal fibers radiate from all angles to the center of the body and converge into a central tendon which is the inferior attachment or muscular skeletal point.
The diaphragm has a dome-like structure with the peripheral segment attached to the chest wall and abdominal cavity. The muscle fibers from these attachments converge in a central tendon, which forms the crest of the dome. The periphery of the diaphragm is made of strong muscular fibers that have their origin from the surroundings of the inferior thoracic aperture. These muscle fibers than converge and insert into the central tendon.
Surgical Considerations
Diaphragmatic Hernia
A diaphragmatic hernia is a congenital disability that occurs when one or more of a person's abdominal organs (stomach, spleen, liver, intestines) move upward into the chest through a defect in the diaphragm. It is usually congenital but can be acquired. Congenital hernias are considered a medical emergency and require prompt surgery.[6]
Congenital Diaphragmatic Hernia (CDH)
A CDH is an abnormal development of the diaphragm during fetal life. The herniation leads to the passage of one or other abdominal organ in the chest leading to the pulmonary hypoplasia which is usually unilateral. The most common subtype of congenital diaphragmatic hernias is Bochdalek Hernia. Other types include Morgagni a hernia, diaphragm eventration, and central tendon defects of the diaphragm.
Acquired Diaphragmatic Hernia (ADH)
An ADH happens due to penetrating or blunt injury. Falls and motor vehicle accidents are major causes of blunt injury while stabs and gunshot wounds lead to penetrating injuries. Penetrating injuries are the more common cause than the blunt injuries as a cause of the diaphragmatic rupture. Further, there can be accidental damage to the diaphragm from the surgical causes. Infrequently, a diaphragmatic hernia may result without any identifiable cause and remain undiagnosed for an undetermined amount of time, until the herniation of abdominal organs in the chest start to cause symptoms.[7]
Treatment
Both acquired, and congenital diaphragmatic hernias usually require immediate surgery. Surgery requires the return of the abdominal organs from the chest cavity back into their original location in the abdominal cavity. The diaphragm should be repaired with staples or permanent sutures with or without a prosthetic patch.
Clinical Significance
The diaphragm has 3 major openings and 5 minor openings.
Major
- The vena caval trunk lies at the level of the T8 vertebra in the central tendon. It allows passage of Inferior vena cava and some branches of the right phrenic nerve.
- The esophageal hiatus lies at the level of the T10 vertebra in a sling of muscle fibers derived from the right crus at the left of the median plane. It allows passage of esophagus, the right and left vagus trunks, the esophageal branches of the left gastric vessels, and the lymph vessels.
- The aortic hiatus lies anterior to the body of the T12 vertebra between the crura. It allows passage of aorta, thoracic duct, and azygos vein.
Minor
- The lesser aperture of right crus (permits lesser and greater splanchnic nerves)
- The lesser aperture of left crus (permits hemiazygous vein; and lesser and greater splanchnic nerves)
- The sympathetic trunk runs posteriorly below the medial lumbocostal arches.
- Foramen of Morgagni is found in the areolar tissue between the sternal and costal part of diaphragm contains the superior epigastric branch of the internal thoracic artery and the lymphatics of the abdominal wall.
- The medial and lateral lumbocostal arches can contain areolar tissue that, when present, separates the superior and posterior surface of a kidney from the pleura.
The figure below shows the openings in the diaphragm: A=vena cava, B=esophagus, C=aorta. The muscular diaphragm surrounds the central tendon in the periphery.
Other Issues
The diaphragm has many other roles besides respiration. It acts as a barrier between the thoracic and abdominal cavity and prevents herniation of abdominal organs into the chest cavity.
Both penetrating and blunt trauma can injure the diaphragm. A tear or rupture of the diaphragm is often a difficult diagnosis. Options for diagnosis include laparoscopy, thoracoscopy or a CT scan. Irrespective of the size of the tear, the muscle must be repaired as soon as possible to prevent herniation of abdominal organs.
The diaphragm is also involved in hiccups. When the muscle is irritated, it can result in sudden contractions which can be uncomfortable. Most hiccups are short-lived, but in rare cases, hiccups may last for a day. If the hiccups persist, they can interfere with breathing.
Media
(Click Image to Enlarge)
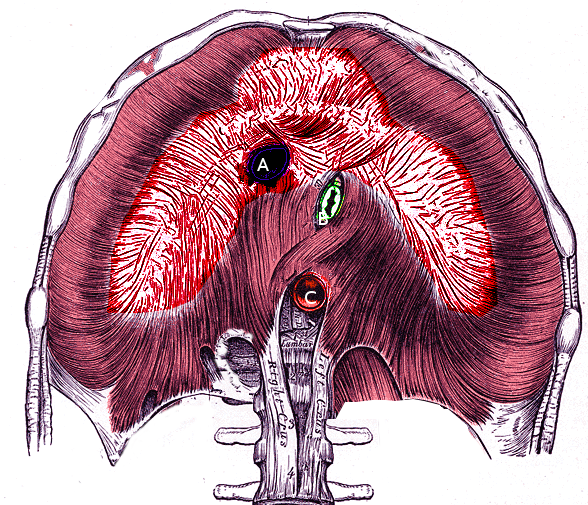
Diaphragm and its apertures
Image courtesy S Bhimji MD
References
Oliver KA, Ashurst JV. Anatomy, Thorax, Phrenic Nerves. StatPearls. 2023 Jan:(): [PubMed PMID: 30020697]
Bordoni B, Purgol S, Bizzarri A, Modica M, Morabito B. The Influence of Breathing on the Central Nervous System. Cureus. 2018 Jun 1:10(6):e2724. doi: 10.7759/cureus.2724. Epub 2018 Jun 1 [PubMed PMID: 30083485]
McCool FD, Manzoor K, Minami T. Disorders of the Diaphragm. Clinics in chest medicine. 2018 Jun:39(2):345-360. doi: 10.1016/j.ccm.2018.01.012. Epub [PubMed PMID: 29779594]
Sefton EM, Gallardo M, Kardon G. Developmental origin and morphogenesis of the diaphragm, an essential mammalian muscle. Developmental biology. 2018 Aug 15:440(2):64-73. doi: 10.1016/j.ydbio.2018.04.010. Epub 2018 Apr 19 [PubMed PMID: 29679560]
Fayssoil A, Behin A, Ogna A, Mompoint D, Amthor H, Clair B, Laforet P, Mansart A, Prigent H, Orlikowski D, Stojkovic T, Vinit S, Carlier R, Eymard B, Lofaso F, Annane D. Diaphragm: Pathophysiology and Ultrasound Imaging in Neuromuscular Disorders. Journal of neuromuscular diseases. 2018:5(1):1-10. doi: 10.3233/JND-170276. Epub [PubMed PMID: 29278898]
Petrosyan M, Shah AA, Chahine AA, Guzzetta PC, Sandler AD, Kane TD. Congenital paraesophageal hernia: Contemporary results and outcomes of laparoscopic approach to repair in symptomatic infants and children. Journal of pediatric surgery. 2019 Jul:54(7):1346-1350. doi: 10.1016/j.jpedsurg.2018.07.008. Epub 2018 Jul 20 [PubMed PMID: 30072216]
Newbury A, Dorfman JD, Lo HS. Imaging and Management of Thoracic Trauma. Seminars in ultrasound, CT, and MR. 2018 Aug:39(4):347-354. doi: 10.1053/j.sult.2018.03.006. Epub 2018 Mar 26 [PubMed PMID: 30070227]