
Introduction
Corneal abrasions, also commonly referred to as a scratched cornea or scratched eye, are one of the most common eye injuries. A scratched cornea often causes significant discomfort, foreign body sensation, severe pain, eye erythema, light sensitivity, and photophobia.[1] Corneal abrasions result from a disruption or loss of cells in the top layer of the cornea, called the corneal epithelium. These types of abrasions are caused by nonpenetrating trauma to the corneal epithelium, which makes up a large percentage of ocular injuries seen in the hospital emergency departments and by primary care physicians.[2]
Corneal abrasions can be classified as traumatic, foreign body-related, fingernail-induced, contact lens-related, or spontaneous.[3][4][5][6][7] Most patients with uncomplicated superficial corneal abrasions recover completely after 3 to 5 days.[8]
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
Corneal abrasions most commonly result after superficial trauma to the eye. The majority of cases are due to minor accidental trauma by a poked finger, fingernail, tree branches, paper, makeup brushes, workplace debris, sports equipment, soap, detergents, etc.[9] Sand, foreign bodies, and other small particles can cause corneal abrasions, especially if the eyes are rubbed.[4]
Damaged contact lenses, malpositioned, dried, or prolonged use of soft or hard contact lenses may increase the risk of a scratched cornea.[3] Abrasions with contact lenses usually occur when they are removed or torn due to excessive use and dryness. Overnight and extensive use of contact lenses can favor corneal abrasions and infection, especially by Pseudomonas aeruginosa, which can lead to severe keratitis and other sight-threatening ocular conditions if not diagnosed and treated appropriately.[10]
Corneal abrasions can be spontaneous and recurrent without signs of trauma. These types of corneal lesions, known as corneal erosions, are more likely to occur in patients with corneal dystrophies, certain systemic conditions that favor dry eye disease, and precedent corneal abrasions.[11][12][13][14] The patients usually complain of acute unilateral sharp pains upon awakening. Corneal erosions are favored by conditions that loosen or weaken the adhesive forces of the layers of the epithelium from the underlying corneal layers.[15]
Epidemiology
Corneal abrasions are common eye injuries across all age groups. They are widespread in the workplace, with an annual incidence of 15 per 1000 employees in US auto workers. About one-quarter of corneal abrasions happen while working, occur more frequently in men, and typically affect patients of 25 to 35 years, probably due to younger men undertaking riskier jobs, having less experience, and tending to disregard safety measures and eye protection.[8] Risk factors in work-related corneal abrasions incidents include a history of trauma (eg, chemical burns, foreign bodies, blunt trauma, radiation exposure), a job in manufacturing or construction, poor or lack of eye protection, and contact lens use.[8] The Bureau of Labor Statistics reported in 2008 that about 60% of facial injuries needing at least one day of sick leave were due to eye-related trauma caused by corneal foreign bodies (34%), corneal abrasions (15%), and chemical burns (10%).[8]
In primary care clinics, eye complaints are responsible for 2% of visits with traumatic conditions; foreign bodies are the reason for 8% of these visits.[16] Epidemiology studies in the United States have reported that these preventable ocular injuries due to accidental ocular foreign bodies and corneal abrasions have an incidence of 2 and 3 cases per 1000 patients, respectively.[17] Results from a study on patients visiting the ER with corneal abrasion in the United Kingdom showed that 64% of those corneal abrasions were due to a reported direct minor trauma.[18]
About 45% of eye-related diagnoses in ER visits are due to corneal abrasions and one-third to foreign bodies.[19] For patients presenting to the ER for foreign body sensation, study results have shown that about 65% of cases had an actual ocular foreign body, while about 13% had corneal abrasions.[20]
A common cause of corneal abrasions is contact lens use. Over 140 million people worldwide use contact lenses for myopia control, refraction, and therapeutic reasons.[21] Corneal abrasions can result from incorrect or malpositioned lens insertion, rubbing, and mechanical forces to the eyelids and foreign bodies between the lens and corneal epithelium.[22] Study results have shown that more than 10% of corneal abrasions in the ER were contact-lens related.[18] Patients presenting to the emergency department with trauma due to contact lenses reported corneal abrasions, epithelium staining, and superficial corneal defects in 87% of cases.[23]
Pathophysiology
Damage to the corneal surface induces changes in the interface between the corneal cells, neighboring cells, and the matrix.[11] Knowledge of the main concepts of the anatomy of the cornea is essential for better understanding the pathophysiology of corneal abrasions. The cornea is an avascular transparent structure (see Image. Cornea Diagram) that provides protection and a barrier against trauma, infection, and damage, contributing to about 70% of the refractive components of the eye (ranging from 40-44 D of refractive power).[24] The average diameter is 10 to 12.5 mm, with central corneal thickness in normal eyes that range from 550 to 565 microns.[25]
The cornea has acellular and cellular components. The cells include keratocytes, epithelium cells, and endothelium cells. The acellular components include glycosaminoglycans and collagen. The cornea comprises layers, including the external epithelium layer, Bowman membrane, stroma, Descemet membrane, and the inner single endothelium layer (see Image. Cornea Layers). Corneal abrasions tend to be superficial and occur in the epithelium, which comprises about 5 to 7 layers of cells. The cornea has a total diameter of about 50 microns, including single-layered basal, winged, and superficial cells.[26] The surface is uniform, smooth, transparent, and made up of stratified nonkeratinized squamous epithelium in direct contact with the overlying tear film.[27] Cells are sealed in the superficial cornea to form a protective barrier by tight junctions between cells.[28]
The typical lifespan for corneal epithelium cells tends to be less than 10 days, and the continuous turnover results from apoptosis, involution, and desquamation.[29] Basal cells and stem cells located in the corneoscleral limbus area are capable of mitosis and give rise to the wing and superficial cells of the cornea.[30] Cells within the epithelium layer synchronize the cornea's homeostasis, equilibrium, and wound healing through proliferation, differentiation, movement, and desquamation.[31] Corneal nerves generate from the trigeminal ganglion (ophthalmic branch) and form nerve-ending ramifications in the epithelium corneal layers, and are essential for the sensation of stimuli and to detect the presence of potentially nocive agents (chemical, mechanical, and thermal). Corneal nerves are also fundamental in producing neurotrophins, proper homeostasis, and corneal repair.[32] Many immune cells reside in the cornea, including lymphocytes, Langerhans cells, innate lymphoid cells, macrophages, and mast cells, which provide immunoregulatory protection and adaptive immunity. These immune components are of utmost importance in this avascularised tissue.[33]
Trauma that causes corneal abrasions activates a dynamic and complex wound-healing process involving migration, cell death, apoptosis, proliferation, cell differentiation, and remodeling of the extracellular matrix.[34]
Thoft and Friend first proposed the X, Y, and Z hypothesis of corneal homeostasis; this involves continuous proliferation and differentiation of active basal cells in the corneal epithelium (X), in addition to the peripheral centripetal movement (Y), coupled with the desquamation of superficial cells (Z) from the superficial cornea.[35]
The wound healing process of corneal abrasions includes the lag phase (damaged cells undergo apoptosis, and the cells and matrix reorganize); cell migration (epithelium cells near the wound flatten and move close to the wounded area); proliferation (mitosis in stem cells increases to amplify cell line); and cellular adhesion (the reorganized epithelium layers form strong adhesions to underlying basal membrane and stroma).[34] Immune cells and corneal nerves play active roles in orchestrating these phases of wound healing.[36][37] Numerous factors are activated in response to trauma and corneal abrasions, including keratin, growth factors, cytokines, basement membrane proteins, integrins, gap junction proteins, endostatin, and thrombospondin.[38]
History and Physical
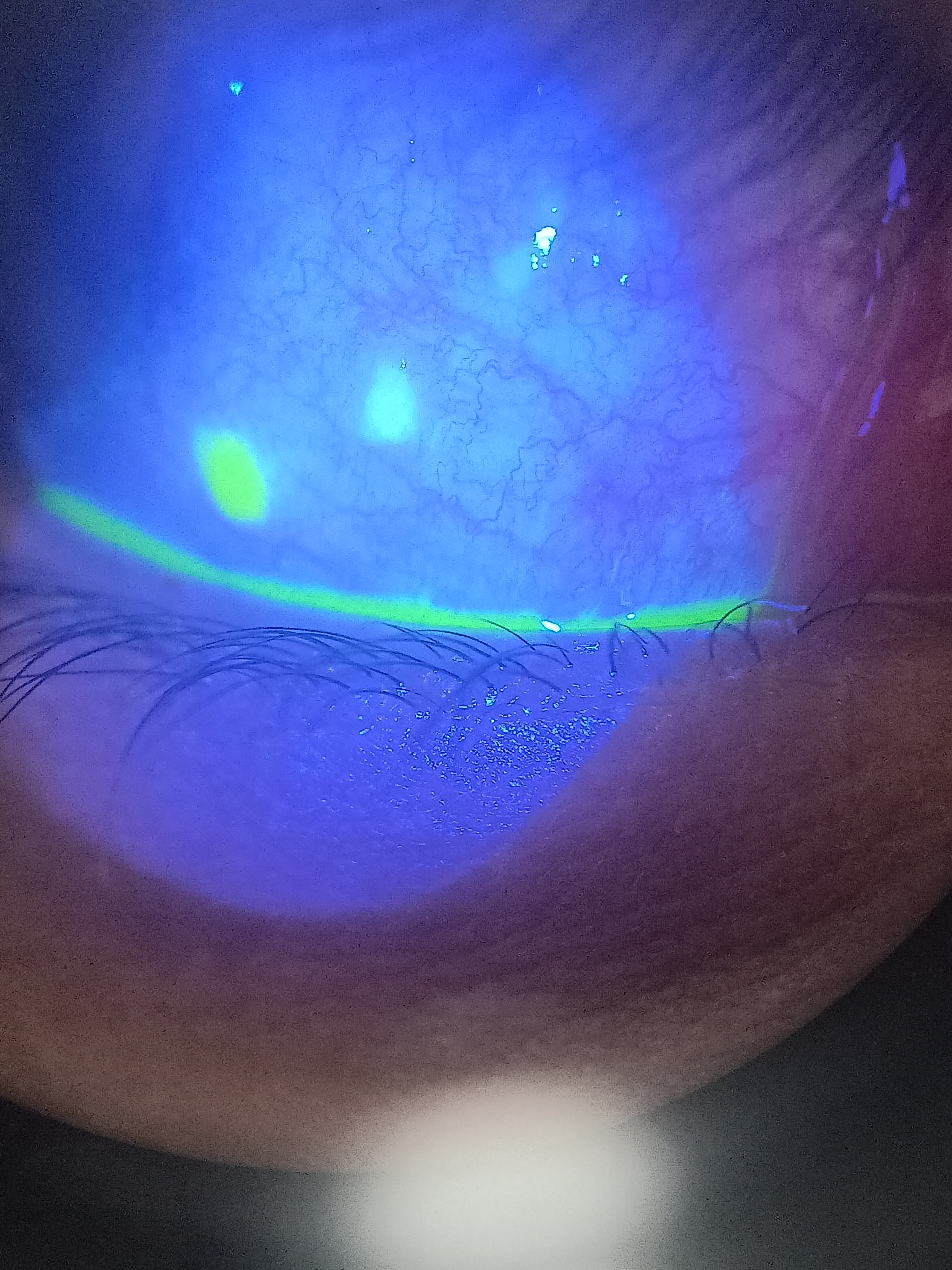
Difficulty opening the eye, photophobia, and foreign body sensation associated with eye pain can be due to a corneal injury.[1] Eye injuries are often not reported. It is important to ask if the patient works with wood or metal because small pieces can get caught under the eyelid and cause injury to the cornea. Corneal abrasions can be associated with redness, light sensitivity, excessive lacrimation, and decreased visual acuity on exam.[39] Fluorescein staining is the most helpful clinical tool to assess corneal abrasion.[40] The dye will get caught in the corneal abrasion and fluoresce under cobalt blue light (see Image. Corneal Lesion).
Symptoms of Corneal Abrasions
- Pain
- Foreign body sensation
- Excessive squinting
- Reflux tear production, watering, tearing
- Photophobia, light sensitivity
- Red eye
- Decreased visual acuity
- History of trauma
Signs of Corneal Abrasions
- Corneal defect stained with fluorescein (see Image. Corneal Lesion)
- Injection of the bulbar conjunctiva
- Corneal sub-edema
- Hyperemia of ciliary vessels
- Induced pupillary meiosis
- Hyphema for severe trauma
- Hypopyon in the presence of intraocular infection
Causes of Corneal Abrasions
- Trauma
- Poked finger or nail scratch
- Makeup
- Tree branches or plants
- Small foreign bodies and debris
- Hard or soft contact lenses
- Chemical or detergent splashes
- Aggressive eye rubbing
- Radiation burns
- Trichiasis
Prevention of Corneal Abrasions
- Use protective eyewear (googles, glasses, shields, helmets, etc)
- Avoid excessive rubbing of the eye
- Proper hygiene and washing of the periorbital and lid region, especially in the presence of dust or debris
- Avoid the use of contact lenses
- Proper contact lens use, cleaning, and fitting
- Artificial tear drops for dry eyes
Evaluation
The clinician can start the eye exam with a penlight if the patient is in severe pain and has difficulty positioning on the slit lamp. An abnormally shaped pupil could be a sign of globe rupture. Topical anesthetics are helpful to facilitate the examination. The conjunctival injection is typically present. A corneal opacity or infiltrate may occur with corneal ulcers or infection. A hazy cornea is a sign of edema from excessive rubbing or epithelium stroma damage. The anterior chamber should be inspected for hyphema or hypopyon. The presence of hyphema or hypopyon requires an immediate ophthalmologic referral. Abrasions over the center of the cornea will cause a decrease in visual acuity. Significant reductions in visual acuity require referral to an ophthalmologist. Abnormal extraocular movement should also be noted.
Fluorescein staining helps identify a corneal epithelial defect.[41] Apply a drop of a topical anesthetic into the eye or on a fluorescein strip and then apply it to the conjunctiva. The fluorescein dye passes over normal cornea tissue but gets stuck in any cornea defects.[42] The dye appears green under cobalt blue light in the presence of denuded epithelium (see Image. Conjunctival Congestion). Traumatic corneal abrasions typically have linear or geographic shapes. If a patient wears contact lenses, the abrasion may have several punctate lesions that coalesce into a round, central defect. Herpes keratitis has dendritic dye uptake (see Image. Corneal Lesion), which requires immediate treatment.[43] Foreign bodies on the inner eyelid typically cause vertical linear corneal lesions; therefore, everting the eyelids is necessary to assess for foreign bodies.[44]
Treatment / Management
The administration of topical antibiotics and cycloplegics have been the mainstay of therapy, along with daily follow-up until the eye heals. Patching was previously routine but is no longer recommended for most patients, especially if contact lenses caused the corneal abrasion.[45] Tetanus prophylaxis is only necessary for penetrating eye injuries and not needed for superficial corneal abrasions.[46](A1)
If a corneal foreign body is detected, attempt to remove the foreign body with a swab or irrigation with saline under direct visualization. Flip the lid and remove any foreign bodies.[47] A metal instrument may be needed if irrigation or a cotton swab fails to remove the foreign body. A topical anesthetic should be instilled (ie, topical oxybuprocaine). Use a 25-gauge needle, hypodermic needle, number 15 blade, or an eye spud to remove the object.[47] If the metal instrument fails, the patient needs an ophthalmology referral for foreign body removal within 24 hours. Topical antibiotics should then be initiated (erythromycin).
Several antibiotic options exist.[48] Ointment formulations provide lubrication to the injured eye. Contact lens wearers will need coverage for Pseudomonas with a fluoroquinolone or aminoglycoside.[49] Erythromycin ointment is applied 4 times daily for 5 days for non-contact lens-wearing patients. Drops are available for sulfacetamide 10%, polymyxin/trimethoprim, ciprofloxacin, or ofloxacin. Avoid aminoglycoside antibiotics in non-contact lens-wearing patients. Duration of therapy is variable, but a patient can discontinue therapy entirely if the eye is symptom-free for 24 hours. Continued symptoms beyond 3 days warrant evaluation by an ophthalmologist. Never use topical corticosteroids due to delayed healing and increased risk of infection.[50][51](A1)
Minor abrasions (less than 4 mm) rarely require analgesia. Control mild to moderate pain with oral nonsteroidal anti-inflammatory drugs (NSAIDs). Ophthalmic topical NSAID solutions provide pain relief.[50](A1)
A few patients with minor abrasions that fail to heal despite these treatments may require oral opioid medications (eg, 2 days of oxycodone prescription should be adequate). Cycloplegic medications can relieve photophobia. Like the opiate medications, 2 days of cycloplegic drops should be enough to manage the photophobia.[52] There are side effects to cycloplegics, such as difficulty with reading. If using a cycloplegic agent, cyclopentolate is a good choice because of its short duration of action.[53](A1)
Differential Diagnosis
Acute pain, blurred vision, photophobia, eye redness, and foreign body sensation are common findings in patients seeking urgent ophthalmic care. The differential diagnosis of corneal abrasion includes, but is not limited to, the following:
- Keratoconjunctivitis
- Dry eye syndrome
- Acute angle-closure glaucoma
- Uveitis
- Infective keratitis (bacterial, fungal, herpetic)
- Corneal ulcer
- Recurrent erosion syndrome
- Trauma
- Neurotrophic exposure keratopathy
- Postoperative complications
- Limbal stem cell deficiency
- Trichiasis
- UV or chemical keratitis
Prognosis
The prognosis is usually excellent if treatment is prompt. However, untreated corneal abrasions can lead to severe infection and permanent scarring blindness.[54] Small corneal abrasions usually completely heal without difficulty in less than 5 days. More extensive abrasions, visual disturbance, and abrasions caused by a contact lens will require close outpatient monitoring by an ophthalmologist. Deep abrasions in the central visual axis heal but leave a scar. In such cases, a permanent loss of visual acuity may result from corneal cloudiness or irregular corneal astigmatism. Recurrent corneal erosions can occur in eyes with previous corneal abrasions, especially in the presence of coexisting corneal dystrophies (ie, epithelium basement membrane dystrophy, lattice degeneration, band keratopathy), prior ocular surgery (refractive, cataract, retinal procedure), dry eye disease, etc.[11]
Complications
Minor corneal abrasions usually heal without difficulty but more extensive abrasions cause the following complications:
- Corneal ulcers
- Bacterial keratitis
- Recurrent erosion syndrome
- Corneal stromal scarring
- Traumatic iritis
Consultations
Urgent follow-up with an ophthalmologist should be performed in the following cases:
- Open-globe injuries require immediate ophthalmology involvement
- Hyphema, hypopyon, and decreased visual acuity (more than 2 lines from the good eye on the Snellen chart) require urgent ophthalmologic follow-up
- Subacute follow-up with ophthalmology for corneal abrasions not healed after 4 days
Deterrence and Patient Education
People who work in high-risk occupations, participate in contact sports, and those whose work or recreation increases the risk of corneal abrasion or ultraviolet light exposure should wear protective eyewear. Patients wearing contact lenses should ensure they fit correctly and replace them as instructed. The eye should not be rubbed after a foreign body injury as it may damage the cornea more. More significant corneal abrasions indicate follow-up visits with an ophthalmologist.
Pearls and Other Issues
Most corneal abrasions heal regardless of therapy within 3 days. Vision should return to normal at that time, although antibiotic ointment formulations may cause an iatrogenic decrease in vision.
Examine contact lens wearers who present with a corneal epithelial defect to look for a corneal infiltrate, a white spot or opacity, or an ulcer, representing a surface breakdown, thinning, or necrosis that occurs in an infiltration area. An ophthalmologist should see any patient with such a finding on the same day. An ointment (erythromycin ophthalmic ointment) is better than drops because it functions as a lubricant and may reduce the disruption of the remaining and newly generated epithelium. Ointments are preferred to drops in children because they do not sting during application.
Due to the risk of sight-threatening bacterial keratitis, patients with corneal abrasions and a history of recent contact lens wear but without a corneal infiltrate receive timely topical antibiotics that are effective against Pseudomonas species (such as the fluoroquinolone class). These patients warrant timely referral to an ophthalmologist or optometrist for daily follow-up care. Patients with uncomplicated, minor, traumatic, or foreign-body corneal abrasions should not undergo patching.
For managing pain in minor corneal abrasions (circular abrasion with a diameter of 4 mm or less), oral analgesics like ibuprofen or an acetaminophen-oxycodone combination, along with or without topical nonsteroidal anti-inflammatory ophthalmic drops (eg, ketorolac), are usually adequate. Significant abrasions can require oral opioid analgesia (eg, acetaminophen-oxycodone combination), cycloplegic drops, and eye patching in selected patients such as those with abrasions covering more than 50% of the corneal surface. Most small corneal abrasions heal within 24 to 48 hours. Older children, adolescents, and adults may only need follow-up if symptoms resolve and healthcare providers provide anticipatory guidance.
Eyelids should be closed with adhesive strips to avoid corneal abrasions in patients who undergo surgery with general anesthesia, especially if the patient suffers from dry eye and the surgical procedure is long because the partial aperture of the lids can favor corneal dryness and abrasion upon waking from surgery.
Indications for urgent referral to an ophthalmologist (after initial treatment) include the following:
- Larger epithelial defects at 24 hours
- Purulent discharge
- Decrease in vision of more than 1 to 2 lines (20/20 to 20/60)
- Corneal abrasions that have not healed after 3 to 4 days
- Children who are unwilling to open the affected eye after 24 hours
Enhancing Healthcare Team Outcomes
Corneal abrasions are a common injury typically seen in urgent care centers and emergency departments. Most of the time, they will heal independently with topical antibiotics to prevent infection. Identifying signs of more severe injury that would necessitate urgent ophthalmologic follow-up is essential. The most dangerous injury is an open globe. It is also important to get a follow-up within 24 hours for large abrasions or decreased visual acuity.[55]
Regions of the country that do not have ophthalmology coverage available will need to establish follow-up or have a low threshold for transferring to a tertiary care center. Daily follow up by an ophthalmic nurse or an ophthalmologist is required for s abrasions, abrasions from the contact lens, abrasions associated with decreased vision, and abrasions in young children. Most small corneal abrasions heal within a few days, and full recovery is expected. Large corneal lesions may take some time to heal, but visual recovery is not always guaranteed.[56]
Collaboration and communication with colleagues, staff, and patients in diagnosing, treating, and managing patients with acute ophthalmologic disorders are key elements for a good outcome. The interprofessional care provided to the patient must use an integrated care pathway combined with an evidence-based approach to planning and evaluating all joint activities. When signs, symptoms, and treatments of complications are identified early, the prognosis and outcomes of patients tend to be better.
Media
(Click Image to Enlarge)
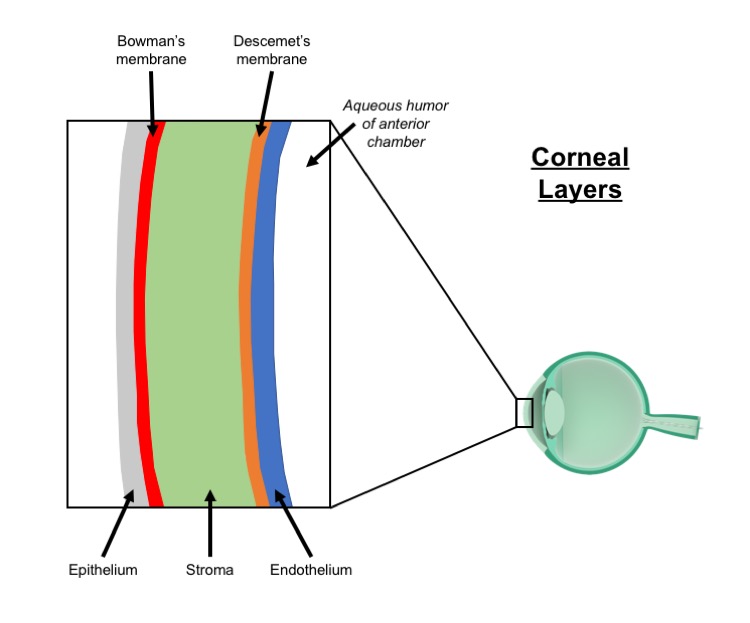
Cornea Diagram. Schematic of cornea (not to scale).
Contributed by Parker Ludwig
(Click Image to Enlarge)
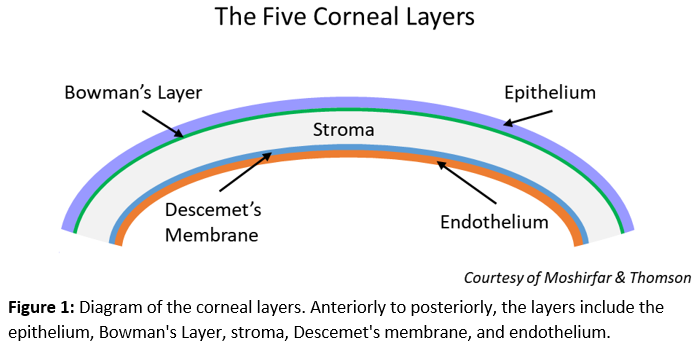
Corneal Layers
Contributed by Moshirfar & Thomson
(Click Image to Enlarge)
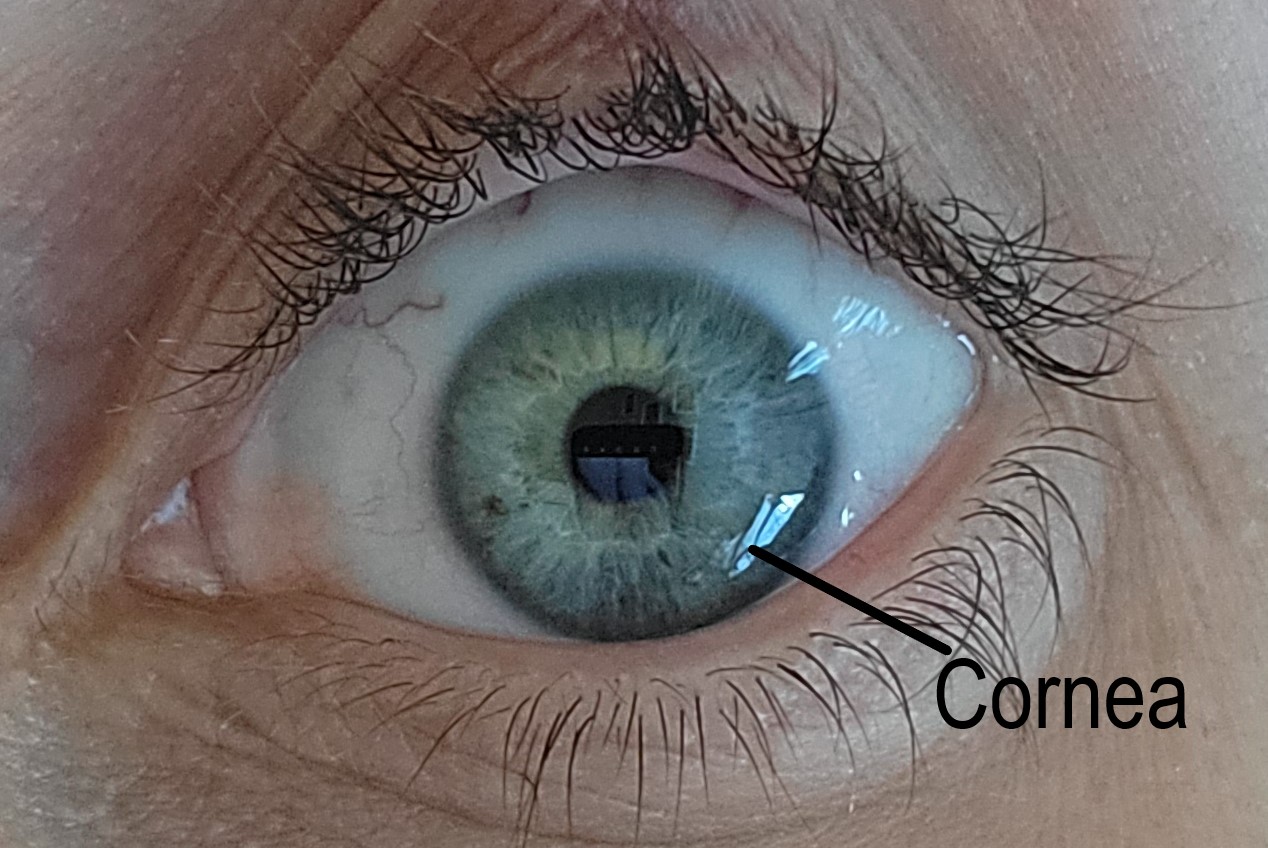
Normal Cornea. A normal cornea that is transparent, avascular, and acts as a barrier to infection.
Contributed by Gary Legault, MD
(Click Image to Enlarge)
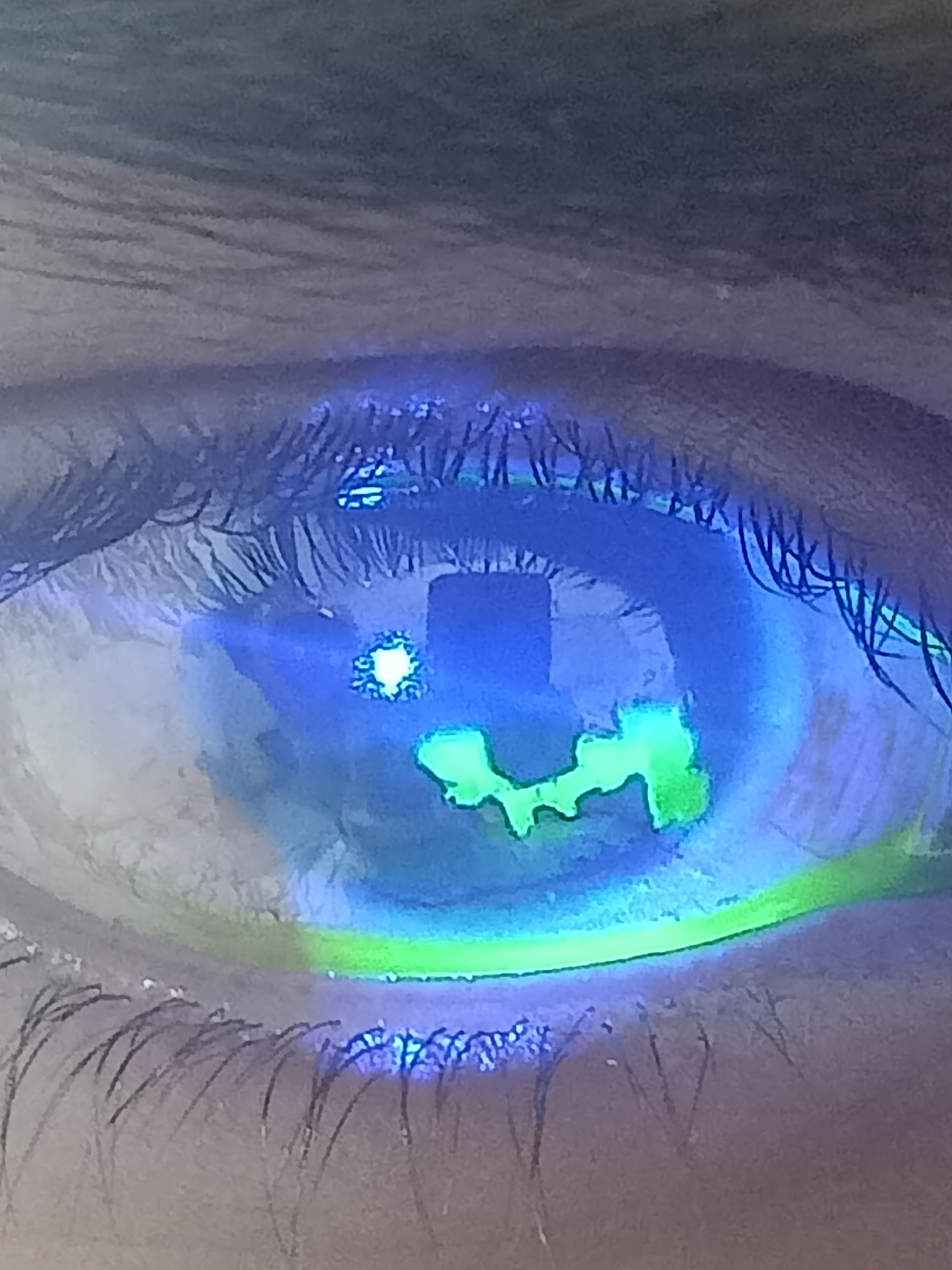
Corneal Lesion. Digital image of the patient depicting a fluorescein-stained lesion.
Contributed by Kirandeep Kaur, MD
(Click Image to Enlarge)
Conjunctival Congestion. Digital image of the patient depicting 2 fluorescein-stained lesions in the conjunctiva along with conjunctival congestion.
Contributed by Bharat Gurnani, MD
References
Sliwicki AL, Orringer K. Corneal Abrasions. Pediatrics in review. 2023 Jun 1:44(6):343-345. doi: 10.1542/pir.2022-005537. Epub [PubMed PMID: 37258882]
Aalam W, Barry M, Alharbi M, Tamur S, Wazzan A, Edward DP. Diagnosis and Management of Corneal Abrasion Perception of (Primary Health Care Physicians and Emergency Physicians) and its Determinants in Saudi Arabia - A Survey. Middle East African journal of ophthalmology. 2021 Jul-Sep:28(3):151-158. doi: 10.4103/meajo.meajo_96_21. Epub 2021 Dec 31 [PubMed PMID: 35125796]
Level 3 (low-level) evidenceWipperman JL, Dorsch JN. Evaluation and management of corneal abrasions. American family physician. 2013 Jan 15:87(2):114-20 [PubMed PMID: 23317075]
Ambikkumar A, Arthurs B, El-Hadad C. Corneal foreign bodies. CMAJ : Canadian Medical Association journal = journal de l'Association medicale canadienne. 2022 Mar 21:194(11):E419. doi: 10.1503/cmaj.211624. Epub [PubMed PMID: 35314442]
Lin YB, Gardiner MF. Fingernail-induced corneal abrasions: case series from an ophthalmology emergency department. Cornea. 2014 Jul:33(7):691-5. doi: 10.1097/ICO.0000000000000133. Epub [PubMed PMID: 24831196]
Level 2 (mid-level) evidenceLim CHL, Stapleton F, Mehta JS. Review of Contact Lens-Related Complications. Eye & contact lens. 2018 Nov:44 Suppl 2():S1-S10. doi: 10.1097/ICL.0000000000000481. Epub [PubMed PMID: 29373389]
Hegarty DM, Hermes SM, Morgan MM, Aicher SA. Acute hyperalgesia and delayed dry eye after corneal abrasion injury. Pain reports. 2018 Jul-Aug:3(4):e664. doi: 10.1097/PR9.0000000000000664. Epub 2018 Jun 20 [PubMed PMID: 30123857]
Ahmed F, House RJ, Feldman BH. Corneal Abrasions and Corneal Foreign Bodies. Primary care. 2015 Sep:42(3):363-75. doi: 10.1016/j.pop.2015.05.004. Epub 2015 Jul 31 [PubMed PMID: 26319343]
McGinley TC Jr. Adult Eye Conditions: Common Eye Conditions. FP essentials. 2022 Aug:519():11-18 [PubMed PMID: 35947131]
Ruffin M, Brochiero E. Repair Process Impairment by Pseudomonas aeruginosa in Epithelial Tissues: Major Features and Potential Therapeutic Avenues. Frontiers in cellular and infection microbiology. 2019:9():182. doi: 10.3389/fcimb.2019.00182. Epub 2019 May 31 [PubMed PMID: 31214514]
Miller DD, Hasan SA, Simmons NL, Stewart MW. Recurrent corneal erosion: a comprehensive review. Clinical ophthalmology (Auckland, N.Z.). 2019:13():325-335. doi: 10.2147/OPTH.S157430. Epub 2019 Feb 11 [PubMed PMID: 30809089]
Bourges JL. Corneal dystrophies. Journal francais d'ophtalmologie. 2017 Jun:40(6):e177-e192. doi: 10.1016/j.jfo.2017.05.003. Epub 2017 Jun 3 [PubMed PMID: 28583694]
Lai SC, Wang CW, Wu YM, Dai YX, Chen TJ, Wu HL, Cherng YG, Tai YH. Rheumatoid Arthritis Associated with Dry Eye Disease and Corneal Surface Damage: A Nationwide Matched Cohort Study. International journal of environmental research and public health. 2023 Jan 15:20(2):. doi: 10.3390/ijerph20021584. Epub 2023 Jan 15 [PubMed PMID: 36674338]
Watson SL, Leung V. Interventions for recurrent corneal erosions. The Cochrane database of systematic reviews. 2018 Jul 9:7(7):CD001861. doi: 10.1002/14651858.CD001861.pub4. Epub 2018 Jul 9 [PubMed PMID: 29985545]
Level 1 (high-level) evidenceLin SR, Aldave AJ, Chodosh J. Recurrent corneal erosion syndrome. The British journal of ophthalmology. 2019 Sep:103(9):1204-1208. doi: 10.1136/bjophthalmol-2019-313835. Epub 2019 Feb 13 [PubMed PMID: 30760455]
Shields T, Sloane PD. A comparison of eye problems in primary care and ophthalmology practices. Family medicine. 1991 Sep-Oct:23(7):544-6 [PubMed PMID: 1936738]
McGwin G Jr, Xie A, Owsley C. Rate of eye injury in the United States. Archives of ophthalmology (Chicago, Ill. : 1960). 2005 Jul:123(7):970-6 [PubMed PMID: 16009840]
Aslam SA, Sheth HG, Vaughan AJ. Emergency management of corneal injuries. Injury. 2007 May:38(5):594-7 [PubMed PMID: 16949077]
Level 2 (mid-level) evidenceMcGwin G Jr, Owsley C. Incidence of emergency department-treated eye injury in the United States. Archives of ophthalmology (Chicago, Ill. : 1960). 2005 May:123(5):662-6 [PubMed PMID: 15883286]
Jayamanne DG. Do patients presenting to accident and emergency departments with the sensation of a foreign body in the eye (gritty eye) have significant ocular disease? Journal of accident & emergency medicine. 1995 Dec:12(4):286-7 [PubMed PMID: 8775960]
Stapleton F, Keay L, Jalbert I, Cole N. The epidemiology of contact lens related infiltrates. Optometry and vision science : official publication of the American Academy of Optometry. 2007 Apr:84(4):257-72 [PubMed PMID: 17435509]
Schornack MM, Nau CB, Harthan J, Shorter E, Nau A, Fogt J. Survey-Based Estimation of Corneal Complications Associated with Scleral Lens Wear. Eye & contact lens. 2023 Mar 1:49(3):89-91. doi: 10.1097/ICL.0000000000000972. Epub 2023 Jan 4 [PubMed PMID: 36602410]
Level 3 (low-level) evidenceLee SY, Kim YH, Johnson D, Mondino BJ, Weissman BA. Contact lens complications in an urgent-care population: the University of California, Los Angeles, contact lens study. Eye & contact lens. 2012 Jan:38(1):49-52. doi: 10.1097/ICL.0b013e31823ff20e. Epub [PubMed PMID: 22157395]
Level 2 (mid-level) evidenceSridhar MS. Anatomy of cornea and ocular surface. Indian journal of ophthalmology. 2018 Feb:66(2):190-194. doi: 10.4103/ijo.IJO_646_17. Epub [PubMed PMID: 29380756]
Feizi S, Jafarinasab MR, Karimian F, Hasanpour H, Masudi A. Central and peripheral corneal thickness measurement in normal and keratoconic eyes using three corneal pachymeters. Journal of ophthalmic & vision research. 2014 Jul-Sep:9(3):296-304. doi: 10.4103/2008-322X.143356. Epub [PubMed PMID: 25667728]
Ruan Y, Jiang S, Musayeva A, Pfeiffer N, Gericke A. Corneal Epithelial Stem Cells-Physiology, Pathophysiology and Therapeutic Options. Cells. 2021 Sep 3:10(9):. doi: 10.3390/cells10092302. Epub 2021 Sep 3 [PubMed PMID: 34571952]
Rocha-de-Lossada C, Torras-Sanvicens J, Peraza-Nieves J. Corneal epithelial cells division assessed by scanning electron microscopy. Indian journal of ophthalmology. 2020 Oct:68(10):2252. doi: 10.4103/ijo.IJO_1214_20. Epub [PubMed PMID: 32971670]
Leong YY, Tong L. Barrier function in the ocular surface: from conventional paradigms to new opportunities. The ocular surface. 2015 Apr:13(2):103-9. doi: 10.1016/j.jtos.2014.10.003. Epub 2015 Jan 13 [PubMed PMID: 25881994]
Altshuler A, Amitai-Lange A, Tarazi N, Dey S, Strinkovsky L, Hadad-Porat S, Bhattacharya S, Nasser W, Imeri J, Ben-David G, Abboud-Jarrous G, Tiosano B, Berkowitz E, Karin N, Savir Y, Shalom-Feuerstein R. Discrete limbal epithelial stem cell populations mediate corneal homeostasis and wound healing. Cell stem cell. 2021 Jul 1:28(7):1248-1261.e8. doi: 10.1016/j.stem.2021.04.003. Epub 2021 May 12 [PubMed PMID: 33984282]
Tavakkoli F, Eleiwa TK, Elhusseiny AM, Damala M, Rai AK, Cheraqpour K, Ansari MH, Doroudian M, H Keshel S, Soleimani M, Djalilian AR, Sangwan VS, Singh V. Corneal stem cells niche and homeostasis impacts in regenerative medicine; concise review. European journal of ophthalmology. 2023 Jul:33(4):1536-1552. doi: 10.1177/11206721221150065. Epub 2023 Jan 5 [PubMed PMID: 36604831]
Liu CY, Kao WW. Corneal Epithelial Wound Healing. Progress in molecular biology and translational science. 2015:134():61-71. doi: 10.1016/bs.pmbts.2015.05.002. Epub 2015 Jun 12 [PubMed PMID: 26310149]
Wilson SE. Corneal wound healing. Experimental eye research. 2020 Aug:197():108089. doi: 10.1016/j.exer.2020.108089. Epub 2020 Jun 15 [PubMed PMID: 32553485]
Liu J, Li Z. Resident Innate Immune Cells in the Cornea. Frontiers in immunology. 2021:12():620284. doi: 10.3389/fimmu.2021.620284. Epub 2021 Feb 26 [PubMed PMID: 33717118]
Ljubimov AV, Saghizadeh M. Progress in corneal wound healing. Progress in retinal and eye research. 2015 Nov:49():17-45. doi: 10.1016/j.preteyeres.2015.07.002. Epub 2015 Jul 18 [PubMed PMID: 26197361]
Thoft RA, Friend J. The X, Y, Z hypothesis of corneal epithelial maintenance. Investigative ophthalmology & visual science. 1983 Oct:24(10):1442-3 [PubMed PMID: 6618809]
Level 3 (low-level) evidenceLiu J, Xiao C, Wang H, Xue Y, Dong D, Lin C, Song F, Fu T, Wang Z, Chen J, Pan H, Li Y, Cai D, Li Z. Local Group 2 Innate Lymphoid Cells Promote Corneal Regeneration after Epithelial Abrasion. The American journal of pathology. 2017 Jun:187(6):1313-1326. doi: 10.1016/j.ajpath.2017.02.010. Epub 2017 Apr 15 [PubMed PMID: 28419818]
Yang L, Di G, Qi X, Qu M, Wang Y, Duan H, Danielson P, Xie L, Zhou Q. Substance P promotes diabetic corneal epithelial wound healing through molecular mechanisms mediated via the neurokinin-1 receptor. Diabetes. 2014 Dec:63(12):4262-74. doi: 10.2337/db14-0163. Epub 2014 Jul 9 [PubMed PMID: 25008176]
Level 3 (low-level) evidenceLoureiro RR, Gomes JÁP. Biological modulation of corneal epithelial wound healing. Arquivos brasileiros de oftalmologia. 2019 Jan-Feb:82(1):78-84. doi: 10.5935/0004-2749.20190016. Epub [PubMed PMID: 30652772]
Hakimi AA, Carter S, Garg S. Detecting corneal injury with a selfie. Academic emergency medicine : official journal of the Society for Academic Emergency Medicine. 2022 Nov:29(11):1403-1404. doi: 10.1111/acem.14577. Epub 2022 Aug 17 [PubMed PMID: 35921203]
Tripathy K. Documentation of corneal epithelial defects with a fluorescein angiographic imaging system. Clinical case reports. 2019 Sep:7(9):1815-1816. doi: 10.1002/ccr3.2350. Epub 2019 Jul 30 [PubMed PMID: 31534763]
Level 3 (low-level) evidenceWilson G, Ren H, Laurent J. Corneal epithelial fluorescein staining. Journal of the American Optometric Association. 1995 Jul:66(7):435-41 [PubMed PMID: 7560732]
Level 3 (low-level) evidenceWilson SA, Last A. Management of corneal abrasions. American family physician. 2004 Jul 1:70(1):123-8 [PubMed PMID: 15259527]
Jamali A, Hu K, Sendra VG, Blanco T, Lopez MJ, Ortiz G, Qazi Y, Zheng L, Turhan A, Harris DL, Hamrah P. Characterization of Resident Corneal Plasmacytoid Dendritic Cells and Their Pivotal Role in Herpes Simplex Keratitis. Cell reports. 2020 Sep 1:32(9):108099. doi: 10.1016/j.celrep.2020.108099. Epub [PubMed PMID: 32877681]
Bhargava M, Bhambhani V, Paul RS. Anterior segment optical coherence tomography characteristics and management of a unique spectrum of foreign bodies in the cornea and anterior chamber. Indian journal of ophthalmology. 2022 Dec:70(12):4284-4292. doi: 10.4103/ijo.IJO_878_22. Epub [PubMed PMID: 36453330]
Kaiser PK. A comparison of pressure patching versus no patching for corneal abrasions due to trauma or foreign body removal. Corneal Abrasion Patching Study Group. Ophthalmology. 1995 Dec:102(12):1936-42 [PubMed PMID: 9098299]
Level 1 (high-level) evidenceBenson WH, Snyder IS, Granus V, Odom JV, Macsai MS. Tetanus prophylaxis following ocular injuries. The Journal of emergency medicine. 1993 Nov-Dec:11(6):677-83 [PubMed PMID: 8157904]
Level 3 (low-level) evidenceGuier CP, Stokkermans TJ. Corneal Foreign Body Removal. StatPearls. 2024 Jan:(): [PubMed PMID: 32119365]
Dang DH, Riaz KM, Karamichos D. Treatment of Non-Infectious Corneal Injury: Review of Diagnostic Agents, Therapeutic Medications, and Future Targets. Drugs. 2022 Feb:82(2):145-167. doi: 10.1007/s40265-021-01660-5. Epub 2022 Jan 13 [PubMed PMID: 35025078]
Clemons CS, Cohen EJ, Arentsen JJ, Donnenfeld ED, Laibson PR. Pseudomonas ulcers following patching of corneal abrasions associated with contact lens wear. The CLAO journal : official publication of the Contact Lens Association of Ophthalmologists, Inc. 1987 May-Jun:13(3):161-4 [PubMed PMID: 3329585]
Level 3 (low-level) evidenceCalder LA, Balasubramanian S, Fergusson D. Topical nonsteroidal anti-inflammatory drugs for corneal abrasions: meta-analysis of randomized trials. Academic emergency medicine : official journal of the Society for Academic Emergency Medicine. 2005 May:12(5):467-73 [PubMed PMID: 15860701]
Level 1 (high-level) evidenceWakai A, Lawrenson JG, Lawrenson AL, Wang Y, Brown MD, Quirke M, Ghandour O, McCormick R, Walsh CD, Amayem A, Lang E, Harrison N. Topical non-steroidal anti-inflammatory drugs for analgesia in traumatic corneal abrasions. The Cochrane database of systematic reviews. 2017 May 18:5(5):CD009781. doi: 10.1002/14651858.CD009781.pub2. Epub 2017 May 18 [PubMed PMID: 28516471]
Level 1 (high-level) evidenceAl-Saleh GS, Alfawaz AM. Management of traumatic corneal abrasion by a sample of practicing ophthalmologists in Saudi Arabia. Saudi journal of ophthalmology : official journal of the Saudi Ophthalmological Society. 2018 Apr-Jun:32(2):105-109. doi: 10.1016/j.sjopt.2017.10.007. Epub 2017 Oct 31 [PubMed PMID: 29942177]
Ball IM, Seabrook J, Desai N, Allen L, Anderson S. Dilute proparacaine for the management of acute corneal injuries in the emergency department. CJEM. 2010 Sep:12(5):389-96 [PubMed PMID: 20880433]
Level 1 (high-level) evidenceSaccomano SJ, Ferrara LR. Managing corneal abrasions in primary care. The Nurse practitioner. 2014 Sep 18:39(9):1-6. doi: 10.1097/01.NPR.0000452977.99676.cf. Epub [PubMed PMID: 25140844]
Jolly R, Arjunan M, Theodorou M, Dahlmann-Noor AH. Eye injuries in children - incidence and outcomes: An observational study at a dedicated children's eye casualty. European journal of ophthalmology. 2019 Sep:29(5):499-503. doi: 10.1177/1120672118803512. Epub 2018 Oct 1 [PubMed PMID: 30270661]
Level 2 (mid-level) evidenceTsai CC, Kau HC, Kao SC, Liu JH. A review of ocular emergencies in a Taiwanese medical center. Zhonghua yi xue za zhi = Chinese medical journal; Free China ed. 1998 Jul:61(7):414-20 [PubMed PMID: 9699394]
Level 2 (mid-level) evidence