
 Heart Failure With Preserved Ejection Fraction (HFpEF)
Heart Failure With Preserved Ejection Fraction (HFpEF)
Introduction
Heart failure is a clinical syndrome resulting from complex pathophysiological processes that impair ventricular structure or function. These impairments prohibit the ventricle from either filling with or ejecting blood.[1] The signs and symptoms of heart failure, particularly dyspnea, fatigue, and congestion, are demonstrative of the most current definition of heart failure—"an inability of the heart to pump blood to the body commensurate with its needs, or to so do only at the cost of increased filling pressures."[1][2]
Heart failure is a significant public health issue; the incidence and prevalence of heart failure are increasing in the United States and across the globe. Additionally, heart failure is the end stage of many disease processes, and the risk of developing heart failure increases with increasing age.[3] Heart failure is frequently a progressive disease process, and progression is associated with decreased survival, regardless of underlying etiology.[1][4] To underline these risks and the progression of disease, the American College of Cardiology and American Heart Association (ACC/AHA) have described and defined the following stages of heart failure:
- Stage A: At Risk for Heart Failure - patients at risk for heart failure without symptoms, structural heart disease, or cardiac biomarkers of (ventricular) stretch or injury. Therapeutic interventions at this stage aim to modify underlying risk factors for the development of heart failure.
- Stage B: Pre-Heart Failure - patients with evidence of increased filling pressures by invasive or noninvasive methods or patients with risk factors and increased biomarkers of stretch or cardiac injury that are not explained by other disease processes. Therapeutic interventions at this stage aim to treat risk and structural heart disease to prevent heart failure.
- Stage C: Symptomatic Heart Failure - patients with structural heart disease with current or previous symptoms of heart failure. Therapeutic interventions at this stage aim to reduce symptoms, morbidity, and mortality.
- Stage D: Advanced Heart Failure - patients with marked symptoms of heart failure that interfere with daily life and with recurrent hospitalizations despite attempts to optimize guideline-directed medical therapy. Therapeutic interventions at this stage aim to reduce symptoms, morbidity, and mortality.[1]
Separate from the ACC/AHA Stage of Heart Failure is the New York Heart Association (NYHA) Classification of Heart Failure. This classification is a subjective assessment by a clinician to characterize the functional capacity and symptoms of patients with ACC/AHA stage C or D heart failure.[1] The NYHA Classification is an independent predictor of mortality and is employed clinically to determine the suitability of therapeutic interventions for patients with stage C or D heart failure.[5][1] The 4 NYHA heart failure classes are as follows:
- Class I: asymptomatic
- Class II: symptomatic with moderate activity
- Class III: symptomatic with mild activity
- Class IV: symptomatic at rest.
Heart failure is further classified by left ventricular ejection fraction (LVEF).[1] The prognosis and response to treatment of patients with heart failure differs significantly when patients are stratified based on LVEF. In 2022, the ACC, AHA, and Heart Failure Society of America (HFSA) released guidelines for the management of heart failure that incorporate the following classification of heart failure by LVEF:
- Heart Failure with Reduced Ejection Fraction (HFrEF): patients with an LVEF ≤40%
- Heart Failure with Improved Ejection Fraction (HFimpEF): patients with a previous LVEF ≤40% and a subsequent measurement of LVEF >40%
- Heart Failure with Mildly Reduced Ejection Fraction (HFmrEF): patients with an LVEF 41% to 49% with evidence of spontaneous or provokable increased left ventricular filling pressures (LVFPs), characterized by elevated natriuretic peptides or hemodynamic measurements. HFmrEF is sometimes referred to as heart failure with midrange ejection fraction in the literature.
- Heart Failure with Preserved Ejection Fraction (HFpEF): patients with an LVEF ≥50% with evidence of spontaneous or provokable increased left ventricular filling pressures (LVFPs), characterized by elevated natriuretic peptides or hemodynamic measurements.[1]
The diagnosis of HFpEF can be challenging, particularly in patients with overt signs or symptoms of congestion.[6] However, approximately 50% of patients with heart failure are classified as HFpEF; not all patients with HFpEF will progress to HFrEF.[7][8] HFpEF is a heterogeneous clinical syndrome with many phenotypes, and the underlying pathophysiological processes of HFpEF differ from those of HFrEF.[9][10] While all patients with heart failure have ventricular diastolic dysfunction, diastolic dysfunction is considered part of the normal again process and is not synonymous with HFpEF.[11]
Patients with HFpEF have increased rates of morbidity and mortality compared to patients without heart failure.[1] However, therapeutic interventions are available to reduce symptoms, improve functional status and quality of life, and reduce hospital admission rates.[12] Clinical understanding of HFpEF continues to evolve, and clinical trials to improve outcomes for patients with HFpEF are ongoing.
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
Heart failure is the common endpoint for many disease processes.[3] Worldwide, the most common underlying etiology of heart failure is ischemic heart disease secondary to coronary artery disease, which confers a relative risk of heart failure of 8.1.[13] Independent risk factors for the development of heart failure as identified during the First National Health and Nutrition Examination Survey (NHANES I) Epidemiologic Follow-up Study include male sex, cigarette smoking, overweight/obesity, diabetes, hypertension, and valvular disease.[13] Social determinants of health, such as education, occupation, and income, also contribute to the development of heart failure.[14][15]
Predisposing Conditions for Primary Heart Failure With Preserved Ejection Fraction
The risk factors, underlying etiologies, and pathophysiology of HFpEF and HFrEF differ significantly; HFpEF is a heterogeneous clinical syndrome.[16] Increasing age is the most significant risk factor for all heart failure subtypes; aging significantly influences the development of HFpEF more than HFrEF.[17][18] However, individuals younger than 65 can develop HFpEF; this may represent a unique age-based phenotype.[9]
This same increased influence is seen for atrial fibrillation, female sex, and pulmonary hypertension of any etiology.[18] Obesity and diabetes are also significant risk factors and predictors of HFpEF.[18] Patients with HFpEF and obesity tend to be younger than patients with HFpEF and an average body mass index.[19] While arterial hypertension is a significant risk factor for the development of HFpEF across all populations, obesity is a disproportionately substantial risk factor for patients who identify as African American or Hispanic.[20]
HFpEF is rarely due to a single identifiable clinical condition but arises in patients with various risk factors; the predominant risk factor may or may not indicate a specific phenotype of HFpEF—thus, the heterogeneity of the disease.[16] Risk factors for the development of HFpEF appear to include but are not limited to:
- Increasing age
- Female sex
- Type 2 diabetes
- Obesity
- Sleep apnea
- Hypertension
- Pulmonary hypertension
- Chronic obstructive pulmonary disease
- Iron deficiency, with or without anemia
- Coronary artery disease
- Atrial fibrillation
- Dysrhythmias [16]
The exact pathogenic role of each risk factor is poorly understood.
Etiologies of Secondary Heart Failure With Preserved Ejection Fraction
Secondary HFpEF occurs in a clinical condition that directly causes the heart to fail. These conditions are sometimes referred to as "HFpEF mimics."[16] These mimics include but are not limited to restrictive and hypertrophic cardiomyopathies of any etiology, constrictive pericarditis, and valvular heart disease.[16][7] In the United States, left-sided valvular disease is the most commonly encountered HFpEF mimic, and aortic stenosis should be suspected in all patients with signs, symptoms, or suspicion of HFpEF.[21][16]
Etiologies of Acute Decompensation of Heart Failure With Preserved Ejection Fraction
Patients with HFpEF are at increased risk for deterioration of cardiac function in the setting of various commonly encountered clinical conditions. The development of a clinical condition requiring increased cardiac output that the failing heart cannot meet increases the risk of acute pulmonary and systemic venous congestion.[22] Examples of cardiovascular and noncardiovascular conditions that may induce the acute decompensation of patients with HFpEF include but are not limited to:
- Acute kidney injury or worsening chronic kidney disease
- Anemia
- Chronic pulmonary disease, or the exacerbation thereof
- Dysrhythmia, particularly tachyarrhythmia, especially new-onset atrial fibrillation
- Infection
- Ischemia
- Increased salt intake or water retention
- Medication noncompliance, including antihypertensive or diuretics
- Poorly controlled or uncontrolled hypertension.
Epidemiology
Heart failure is a significant public health issue in the United States and globally. Worldwide estimates for individuals living with heart failure exceed 60 million people, equating to a prevalence of 1% to 3% of the global population.[17] Heart failure is the most common reason for hospitalization for patients 65 and older in the United States, and rates of hospitalizations increased from 2014 to 2017.[23] Approximately 6.7 million Americans older than 25 are estimated to have some form of heart failure; this number is expected to increase to 8.5 million Americans by 2030.[23] The incidence and prevalence of heart failure increase with age.[17] The lifetime risk of heart failure has increased from approximately 20% to 24%, possibly due to an increase in life expectancy and the incidence of comorbidities such as hypertension, diabetes, and obesity.[24]
Data gathered from the second 25-year epoch of the Framingham Heart Study (1990-2014) has demonstrated that the lifetime risk of HFpEF approximates 19.3%, exceeding the approximate 11.4% lifetime risk of HFrEF.[23][24] This appears to be particularly true for women, whose apparent lifetime risk of HFpEF is 10.7% compared to 5.8% for HFrEF; these risks vary with ethnicity.[25][26]
The incidence and prevalence of HFpEF varies among populations and is increasing overall; this increase may partially be due to improved diagnostic capabilities and more uniform diagnostic parameters. Tsao et al. reported an increase of 53% in HFpEF diagnoses among participants in the Framingham Heart Study and Cardiovascular Health Study between 2000 and 2009.[27] Chang et al. reported an 8.2% increase in HFpEF diagnoses among Black women compared to a 5.9% increase for White women; all patients participated in the Atherosclerosis Risk in Communities Study between 2005 and 2014.[26] The same study demonstrated a rise in HFpEF diagnoses for Black men (5.7%) and White men (6.3%).[26] Contrarily, data derived from Olmstead County in Minnesota demonstrated a decrease of 28% in the incidence of HFpEF diagnoses between 2000 and 2010.[23]
While it is clear that the overall prevalence of heart failure is increasing globally, the incidence and prevalence of heart failure demonstrate significant geographic differences. However, data are lacking from some geographic areas, such as Sub-Saharan Africa, and differences in diagnostic criteria and reporting practices across the globe limit the accuracy of comparative data. Despite these limitations, when available data are derived from studies that define HFpEF as an ejection fraction of ≥50%, stark geographic differences in prevalence emerge. Shiga et al. reported an HFpEF prevalence of 43% in 1245 patients with heart failure hospitalized in Japan between 2013 and 2014.[28] Wang et al. evaluated 5236 patients in a community-based heart failure management program in Australia and reported a 37.4% prevalence of HFpEF diagnoses.[29] In contrast, the prevalence of HFpEF diagnoses in the European Society of Cardiology long-term registry and Asian Sudden Cardiac Death in Heart Failure Registry was only 16%.[30]
Pathophysiology
The clinical manifestations of HFpEF are ultimately due to complex pathophysiological processes in cardiomyocyte structure and function, resulting in hemodynamic derangements.[2] However, the pathophysiology of HFpEF is likely not limited to the cardiomyocyte (see Image. Pathophysiology of Heart Failure).
Obesity is a major risk factor for the development of HFpEF.[31] Obesity is a chronic systemic inflammatory state that induces hemodynamic derangements and hormonal abnormalities that stress the cardiovascular system.[32] Overweight and obese individuals demonstrate subclinical changes in the structure and function of the left ventricle, even in the presence of a normal ejection fraction.[33] Increased adiposity is associated with worsening left ventricular diastolic function regardless of left ventricular mass.[34] Central obesity is associated with age-related increases in ventricular end-systolic elastance in women but not in men; obesity and female sex are significant risk factors for the development of HFpEF.[35] Additionally, right ventricular function is impaired in patients with HFpEF; right ventricular dysfunction is more marked in obese patients with HFpEF than in those with a normal body mass index.[36][37][38]
Integral to the pathophysiology of HFpEF is the concept of diminished physiologic reserve.[2] Abnormalities in skeletal muscle and vascular endothelium significantly contribute to decreased reserve. Exercise tolerance and capacity are decreased in patients with HFpEF, as demonstrated by more severe dyspnea and fatigue at matched workloads than controls.[39] This appears particularly true in older patients with HFpEF.[40][41] Additionally, patients with HFpEF demonstrate impaired peripheral oxygen extraction during exercise; the exact etiology of this impairment remains undefined but may represent intrinsic deficiencies in the function of skeletal muscle, vascular endothelium, or mitochondria.[42][43] Patients with HFpEF demonstrate a reduction in total arterial compliance during submaximal and peak exercise.[44] While oxygen transport and utilization are impaired in all patients with HFpEF regardless of the degree of exercise intolerance, exact impairments vary among patients, and underlying comorbidities strongly influence impairment.[45][42]
While the cellular mechanisms contributing to HFpEF remain ill-defined, the result of cellular and tissue pathophysiologic processes is structural remodeling of the left ventricle, a subsequent decrease in left ventricular reserve, abnormal hemodynamics, and the secondary organ dysfunction that causes the clinical syndrome of HFpEF.[2] Historically, HFpEF was thought to present in patients with concentric ventricular remodeling; recent studies have demonstrated that HFpEF may be observed in patients with any form of cardiac remodeling, and many patients with HFpEF have normal ventricular structure.[46]
Despite the heterogeneity of left ventricular structure, the most prominent hemodynamic finding in patients with HFpEF is elevated LVFPs.[2] Patients in the early stages of HFpEF have normal LVFPs at rest, and elevations only occur with exercise.[47][39] As the disease progresses, elevations in LVFPs are observed at rest.[39] These elevations in LVFPs are the result of left ventricular diastolic dysfunction secondary to incomplete myocardial relaxation, increased ventricular stiffness with subsequent decreased ventricular distensibility, and a shift in the Frank-Starling mechanism initially during exercise and eventually at rest.[48][49][50]
Elevations in LVFPs, even when inconsistent, induce structural remodeling of the left atrium. Significant differences in left atrial structure and function exist between patients with HFpEF and those with HFrEF; left atrial function is more closely correlated with outcomes in HFpEF.[10] Compared to patients with HFrEF, patients with HFpEF have smaller left atrial volumes. However, patients with HFpEF have increased left atrial peak pressures, stiffness, and wall stress and are more likely to have atrial fibrillation.[10] Atrial fibrillation further exacerbates the remodeling and dysfunction of the left atrium, which increases the risk of pulmonary hypertension.[51] The development of pulmonary hypertension significantly increases the risk of death in patients with HFpEF.[52]
The development of pulmonary hypertension increases right ventricular dysfunction, and this phenomenon is increased in patients with obesity who are already at increased risk of right ventricular dysfunction.[2] Right ventricular dysfunction significantly increases the risk of death in patients with HFpEF.[36][53]
Ultimately, it is this constellation of dysfunctional processes at the cellular, tissue, and organ levels that causes the clinical constellation of signs and symptoms observed in patients with HFpEF, namely exertional dyspnea progressing to dyspnea at rest, fatigue, decreased organ perfusion, pulmonary congestion, and edema.[2]
Histopathology
Endomyocardial biopsy is neither required nor routinely recommended when diagnosing or managing chronic HFpEF. However, multiple studies have suggested that, unlike the myocardial remodeling in HFrEF driven by cardiomyocyte loss, cardiac remodeling in HFpEF may stem from coronary microvascular inflammation and deranged intramyocardial signaling.[54] The myocardium of patients with HFpEF demonstrates upregulated E-selectins and intercellular adhesion molecule-1 expression, which may contribute to cardiomyocyte hypertrophy and stiffness.[55] Cardiomyocytes from patients with HFpEF demonstrate increased levels of collagen and titin, which may also contribute to ventricular stiffness.[56] Canine studies have demonstrated that increased phosphorylation of titin improves ventricular diastolic distensibility.[57]
History and Physical
Patients with HFpEF typically exhibit intolerance to physical activity characterized by exertional dyspnea (98%) and fatigue (59%).[2][58] With the progression of HFpEF, these symptoms will occur with lower activity levels and may be accompanied by evidence of congestion.[2][58] Some patients with HFpEF are clinically asymptomatic, or their symptoms are so mild they go unnoticed.
The remaining clinical manifestations of HFpEF are typically the same as seen in other heart failure subtypes, including HFrEF. Obtaining a thorough medical history and performing a comprehensive physical examination facilitate the classification of heart failure, which helps guide therapeutic interventions. The signs and symptoms of heart failure overlap with many other disease processes. Worsening ventricular dysfunction results in more severe symptoms and apparent signs. However, there is no single sign or symptom pathognomonic for heart failure.
Medical History
A comprehensive medical history should include a thorough medication history, including patient medication compliance. Inquiries into cardiovascular risk factors, known cardiovascular diagnoses, and prior cardiovascular interventions are mandatory. Any family history of heart failure in the 3 previous generations should be noted; many cardiomyopathies have a genetic component. Quantification of current and prior tobacco and alcohol use, as well as any history of exposure to drugs of abuse, must be pursued. An assessment of social determinants of health is recommended.[1]
Symptoms that patients with heart failure commonly describe include dyspnea, initially with exertion and then at rest. Patients may describe orthopnea or paroxysmal nocturnal dyspnea.[2][58] Dulled mental status or "brain fog" is not uncommon. Daytime oliguria with resulting nocturia is regularly seen as extravasation of vascular fluid worsens. Peripheral edema of the distal lower extremities may initially resolve with elevation; patients commonly report going to bed with swollen feet that normalize by morning. Eventually, this edema may become pitting. Right upper quadrant pain is sometimes reported and is evidence of liver capsular distention. Anorexia and nausea may be evidence of decreased perfusion of the bowel and bowel edema.[59] Exertional chest pain is also a common presenting symptom.[59]
Physical Examination
Physical examination findings vary with the severity of the heart failure. Patients with isolated HFpEF who are not acutely decompensated are most likely to demonstrate mild systolic hypertension, and approximately 10% to 20% have some degree of jugular venous distention.[58]
Evidence of diaphoresis, tachycardia, tachypnea, and hypoxia are indicative of severe heart failure or acute decompensation.[59] Contrarily, patients with severe decompensation may be hypotensive due to decreased peripheral tissue perfusion.[59] Cardiopulmonary auscultation may reveal rales or an S3 or loud P2 heart sound.[58] Pitting edema of the lower extremities may be observed; presacral pitting edema may be noted in nonambulatory patients. Hepatomegaly may be observed, which may be tender in acute decompensation. A hepatojugular reflex and ascites demonstrable by a fluid wave or changes in abdominal percussion are evidence of significant peripheral congestion.
Evaluation
Exertional dyspnea is a common clinical complaint. The clinical signs and symptoms of heart failure are reported and observed in many disease processes. Additionally, the overt manifestations of HFpEF are common to all subtypes of heart failure, making diagnosing HFpEF challenging.[60] It is reasonable to suspect HFpEF as a possible diagnosis in any patient with exertional dyspnea and one of the following clinical parameters not otherwise explained by an alternative diagnosis:
- Age 60 or older
- Atrial fibrillation[61]
- Chronic kidney disease
- Coronary artery disease
- Diabetes
- Hypertension
- Overweight/obesity [1]
Diagnostic algorithms such as the HFA-PEFF (Heart Failure Association. Pretest Assessment, Echocardiography and natriuretic peptide, Functional testing, Final etiology) and H2FPEF (Heavy, 2 or more hypertensive drugs, atrial Fibrillation, Pulmonary hypertension, Elder older than 60, elevated Filling pressures) have been developed and evaluated to identify HFpEF noninvasively. Additional testing, such as echocardiography and measurement of natriuretic peptides, is required to apply these algorithms and confirm a diagnosis of HFpEF.[60]
An evidence-based diagnostic approach to patients with suspected HFpEF is outlined in the 2022 AHA/ACC/HFSA Guideline for the Management of Heart Failure.[1] For patients presenting with a sign or symptom of HFpEF, additional testing is recommended to establish the diagnosis and, if possible, the specific etiology; the presence of underlying comorbidities should also be determined and documented (see Image. Flowsheet).
Initial Evaluation: Laboratory Testing
Complete blood count: Anemia is an established risk factor for heart failure and negatively affects clinical outcomes; the negative impact is inversely proportional to the hemoglobin level.[62]
Serum electrolytes, including sodium, potassium, calcium, and magnesium: Hyponatremia and hypochloremia are strong adverse prognostic indicators in patients with heart failure.[63]
Serum creatinine and blood urea nitrogen: Chronic kidney disease is an established risk factor for heart failure and negatively affects clinical outcomes; the negative impact is inversely proportional to the estimated glomerular filtration rate (eGFR).[62]
Serum glucose: Diabetes is a common comorbidity and an underlying risk factor for the development of HFpEF.[18]
Fasting lipid profile: Multiple recent studies have suggested that dysregulation of lipid metabolism may contribute to the pathophysiology of HFpEF, HFpEF may alter lipid metabolism, and hypertriglyceridemia may increase the risk of mortality and rehospitalization in patients with HFpEF.[61][64][65]
Liver function tests: Metabolic dysfunction-associated steatotic liver disease (MASLD; previously nonalcoholic fatty liver disease or NAFLD) has been closely demonstrated to increase the development and progression of HFpEF.[66] It has been proposed that several MASLD-associated HFpEF phenotypes are commonly encountered in clinical practice.[66]
Iron studies, including serum iron, ferritin, and transferrin saturation: Intravenous iron therapy in symptomatic, iron-deficient patients with heart failure has been shown to improve functional status and quality of life and reduce hospitalizations for worsening heart failure.[67]
Thyroid-stimulating hormone: Hypothyroid and hyperthyroid states are underlying risk factors for the development of heart failure, and low triiodothyronine syndrome is commonly encountered in patients with HFpEF.[68]
B-type natriuretic peptide (BNP) or N-terminal prohormone of B-type natriuretic peptide (NT-proBNP): Measurement of either natriuretic peptide is helpful to exclude or support a diagnosis of heart failure.[1] No scientific evidence exists to advocate using one test over another; using their respective values and endpoints interchangeably is inappropriate.[1] However, measuring natriuretic peptides in the outpatient setting in patients with dyspnea and an equivocal physical examination provides minimal diagnostic value.[1] Many cardiac and noncardiac conditions can cause elevation in natriuretic peptide levels, including advancing age, atrial fibrillation, and chronic kidney disease.[1]
Initial Evaluation: Noninvasive Testing and Cardiac Imaging
12-lead electrocardiogram (ECG): Electrocardiography is routinely performed to evaluate patients with suspected heart failure to obtain information regarding rate, rhythm, and ventricular conduction.[1]
Chest radiography: A chest x-ray is indicated in the initial evaluation of patients with suspected HFpEF.[69] Chest radiography permits the assessment of the cardiac silhouette and heart size, pulmonary airspaces, vascular congestion, and other thoracic disease processes that may contribute to exertional dyspnea.[1]
Transthoracic Echocardiography (TTE): Echocardiography is perhaps the most helpful tool in diagnosing HFpEF and is strongly recommended.[1] The need to categorize heart failure is considered an indication to perform TTE.[70] Determination of LVEF is the critical step in classifying heart failure and guides evidence-based therapeutic interventions.[1] If TTE is inadequate, other cardiac imaging studies such as cardiac magnetic resonance, cardiac computed tomography, or radionuclide imaging can be considered.[1] However, TTE provides a wealth of information in a noninvasive manner, including the size, function, motion, and geometry of all cardiac chambers and valves, estimates of LVFPs, and estimates of atrial, systolic pulmonary artery, and central venous pressures.
Treatment / Management
Therapeutic Interventions in Heart Failure with Preserved Ejection Fraction
The goals of therapy for HFpEF are to reduce symptoms, improve quality of life, prevent disease progression, reduce hospitalizations, and effectively manage underlying comorbidities. To this end, lifestyle and behavioral modifications are a cornerstone of therapeutic intervention.
Lifestyle interventions
Several studies have demonstrated that exercise training improves cardiorespiratory fitness and quality of life in patients with HFpEF.[71] Exercise training, exercise-based cardiac rehabilitation, and weight loss improve functional status, exercise performance, rates of heart failure-specific hospitalization, and quality of life in patients with HFpEF.[72] Caloric restriction and exercise training may have positive additive effects in patients with HFpEF, especially if they are older with concomitant obesity.[73] In addition to caloric restriction, at least 1 study has demonstrated that sodium restriction as part of the Dietary Approaches to Stop Hypertension (DASH) diet improves ventricular diastolic function and arterial elastance in patients with HFpEF and hypertension.[74](A1)
Antihypertensive therapies
Diuretics, angiotensin receptor–neprilysin inhibitors (ARNIs), angiotensin receptor blockers (ARBs), and mineralocorticoid antagonists (MRAs) are the preferred pharmacologic interventions if blood pressure is uncontrolled in a patient with HFpEF. The currently recommended blood pressure goal is below 130/80 mm Hg.[12] The nonrandomized Optimize-HF (Organized Program to Initiate Lifesaving Treatment in Hospitalized Patients with Heart Failure) registry demonstrated improved 30-day mortality and decreased hospitalization for heart failure with diuretic use compared to no diuretic therapy after hospital discharge for heart failure.[75] Bumetanide and torsemide have better bioavailability than furosemide. Some patients may require a combination of diuretic classes, such as thiazide or thiazide-like diuretics. Diuretic resistance is a common problem and may be due to excessive dietary sodium consumption, using medications that negatively affect diuretic action, such as nonsteroidal anti-inflammatory drugs, or underlying chronic kidney disease.(B3)
A meta-analysis of 11 trials of 14,262 patients in sinus rhythm, including 244 patients with HFpEF, demonstrated that beta blockers reduce mortality and have beneficial effects.[76] Patients with HFpEF and concomitant coronary artery disease also benefit from beta-blocker administration. The Treatment of Preserved Cardiac Function Heart Failure with an Aldosterone Antagonist (TOPCAT) trial was a randomized, double-blind trial of 3445 patients with symptomatic heart failure and an LVEF of greater than 45% that demonstrated some reduction in hospitalization rates for heart failure.[77] This was particularly true for patients with an LVEF of less than 55% to 60% and those with elevated BNP.[78](A1)
A prespecified subgroup analysis of patients in the Prospective Comparison of ARNI with ARB Global Outcomes in HFpEF (PARAGON-HF) demonstrated that sacubitril-valsartan, as compared with valsartan, has a tendency to lower the risk of heart failure-related hospitalizations overall, but more so in women with HFpEF than men; the average LVEF in study participants was 57%.[79]
Sodium-glucose cotransporter 2 inhibitor therapy
The effects of sodium-glucose cotransporter 2 inhibitor (SGLT2i) therapy on cardiovascular mortality and hospitalization in patients with HFpEF has been demonstrated in the Dapagliflozin Evaluation to Improve the Lives of Patients with Preserved Ejection Fraction Heart Failure (DELIVER) and Empagliflozin in Heart Failure with a Preserved Ejection Fraction (EMPEROR-PRESERVED) trials.[80] The DELIVER trial demonstrated that dapagliflozin decreased the risk of worsening heart failure or cardiovascular death among patients with HFpEF.[81] The EMPEROR-PRESERVED trial demonstrated significant reductions in cardiovascular mortality, heart failure-related hospitalizations, decline in kidney function, and improved quality of life in patients with HFpEF.[82] The effects of SGLTi therapy are consistent for patients with HFpEF across all age groups, and increasing age has not been associated with an increase in adverse events.[16][83] SGLT2i therapy should be considered in all patients with HFpEF, with or without underlying type 2 diabetes, as early as index hospitalization after initial medical stabilization.[81]
In patients with HFpEF, obesity, and underlying type 2 diabetes, glucagon-like peptide (GLP-1) analogs or glucose-dependent insulinotropic polypeptide (GIP) receptor antagonists are beneficial if dual therapy is required.[12] (B3)
Rate control in atrial fibrillation
Beta blockers and nondihydropyridine calcium channel blockers are the preferred therapies for rate control in patients with atrial fibrillation and HFpEF. Digoxin may be considered in hypotensive patients. Atrial fibrillation in patients with HFpEF and hypertrophic cardiomyopathy, cardiac amyloidosis, rheumatic mitral valve stenosis, or a mechanical mitral valve requires anticoagulation regardless of CHA2DS2-VASc score. The 2023 ACC/AHA Guideline for the Diagnosis and Management of Atrial Fibrillation recommends catheter ablation as a first-line therapy to improve symptoms of paroxysmal atrial fibrillation in younger patients with fewer comorbidities.[84](A1)
Additional therapies
In patients with HFpEF and suspected sleep apnea, consultation with sleep medicine for possible polysomnography is recommended. Fatigue is a common symptom of heart failure, and daytime sleepiness is a common symptom of sleep apnea; obesity is a risk factor for both disease processes.[1](A1)
Using CardioMEMS, a pulmonary artery pressure hemodynamic monitoring system, improves quality of life and decreases hospitalizations in patients with HFpEF and frequent hospitalizations.[85] Additionally, CardioMEMS utilization has been shown to improve underlying metabolic comorbidities in tandem with improving pulmonary artery pressures.[85]
Coronary angiogram and revascularization should be considered if ischemia is driving symptoms of HFpEF.[86]
The 2022 ACC/AHA Guideline for the Management of Heart Failure recommends that all patients with a diagnosis of heart failure receive palliative and supportive care.[1] In the context of patients with HFpEF, palliative care is defined as "patient- and family-centered care that optimizes health-related quality of life by anticipating, preventing, and treating suffering."[1] Primary palliative care should begin early in the course of illness, and the interdisciplinary team can address many primary needs.[87] Components of primary palliative care include high-quality communication, anticipatory guidance, advance care planning, home and case management assistance, care coordination, and addressing barriers to care such as food insecurity and transportation needs.[1][87][88](A1)
Acute Decompensation of Heart Failure with Preserved Ejection Fraction
Multidisciplinary shock team assessment and intervention can improve 30-day all-cause mortality and reduce in-hospital mortality in patients with clinical and hemodynamics-proven cardiogenic shock of any etiology.[89] Intravenous vasopressor support can temporarily improve hemodynamics in patients with cardiogenic shock and improve end-organ perfusion; norepinephrine is preferred except in patients with tachyarrhythmias who benefit from phenylephrine. Vasopressor support allows time for diuresis and correction of precipitating factors like arrhythmia and ischemia.
Appropriate ventilatory support and diuresis are the cornerstones of therapy for patients with acutely decompensated HFpEF. In most cases, loop diuretics are preferred to thiazide diuretics; there is no scientific evidence to support one loop diuretic over another in acutely decompensated patients with HFpEF. The Diuretic Optimization Strategies Evaluation (DOSE) trial revealed no clinically significant differences in symptomatic improvement between bolus or continuous intravenous loop diuretics.[90] Some patients may require a combination of diuretic classes, such as thiazide, thiazide-like, or acetazolamide. Adding metolazone increases the risk of hypokalemia, hyponatremia, worsening renal function, and mortality compared to loop diuretics alone.[91] Contrarily, the Acetazolamide in Decompensated Heart Failure with Volume OveRload (ADVOR) trial demonstrated that adding acetazolamide to loop diuretics increases the incidence of successful decongestion in patients with acute heart failure within three days compared to placebo.[92](A1)
Following the initial stabilization of hemodynamics and ventilation, assessing and managing ischemia, arrhythmia, and other precipitating factors and comorbidities is paramount. Urgent revascularization is preferred in the setting of acute coronary syndrome. Intravenous or topical nitroglycerin is preferred in patients with hypertensive urgency or emergency and pulmonary edema; nitroglycerin decreases preload in patients with pulmonary edema.
Short-term renal replacement therapy or ultrafiltration should be considered in symptomatic hypervolemic patients with poor renal function and minimal urine output, irrespective of supportive therapy and stable hemodynamics. Patients with poor baseline renal function or end-stage renal disease are at a significantly increased risk for requiring renal replacement therapy.
There is no substantial evidence supporting the early initiation of angiotensin-converting enzyme (ACE) inhibitors, ARBs, ARNIs, MRAs, SGLT2i therapy, or beta blockers to prevent major adverse cardiac events in unstable patients with acutely decompensated HFpEF. Thiazolidinediones and dipeptidyl peptidase-4 (DPP-4) inhibitors such as sitagliptin or saxagliptin are contraindicated in acutely decompensated HFpEF.
Differential Diagnosis
The differential diagnosis of exertional dyspnea with or without generalized fatigue is extensive and includes cardiac and noncardiac etiologies. Additionally, because the clinical syndrome of heart failure is the common endpoint for many disease processes, the overarching differential diagnosis for heart failure is similarly broad. However, in patients with exertional dyspnea and an underlying risk factor for HFpEF or comorbidity strongly associated with the development of HFpEF, the following diagnoses should be considered:[7][16]
- Coronary artery disease
- Hypertension
- Valvular disease, particularly left-sided valvular disease
- Infiltrative cardiac diseases such as amyloidosis, hemochromatosis, and sarcoidosis
- Hypertrophic cardiomyopathy
- Constrictive pericarditis.
Prognosis
Patients with HFpEF have increased rates of morbidity and mortality compared with patients without heart failure. However, recent studies suggest that morbidity rates are similar for patients with HFpEF and HFrEF.[27][93] The presence and severity of common comorbidities such as hypertension, atrial fibrillation, diabetes, and chronic kidney disease significantly influence the prognosis of patients with HFpEF.[27][94][27] Biomarkers like BNP, NT-pro BNP, and high-sensitivity troponin are associated with prognosis in HFpEF; elevated biomarker levels may indicate increased cardiovascular risk.
Independent predictors of mortality in patients with HFpEF confer a poor prognosis.[10][52][36][53][94] These predictors include but are not limited to:
- Older age
- Male sex
- NYHA class C or D
- Lower LVEF and the degree of diastolic dysfunction
- Extent of coronary artery disease
- Peripheral artery disease
- Diabetes
- Functional renal impairment
- Pulmonary hypertension
- Right ventricular dysfunction
- Atrial fibrillation
- Increased red cell distribution width.
Complications
Complications stemming from HFpEF are multifaceted, reflecting the intricate interplay of diverse risk factors, complex pathophysiological processes, and the heterogeneous nature of this clinical syndrome. Left atrial dysfunction, atrial fibrillation, and pulmonary hypertension often develop, placing an increased workload on the right ventricle and increasing the risk of biventricular failure.
Beyond cardiovascular implications, HFpEF introduces complications associated with comorbidities such as obesity, diabetes, and chronic kidney disease. Impaired exercise tolerance and functional decline are common, as diminished physiologic reserve manifests in more severe dyspnea and fatigue, impacting daily activities.
Diagnostic challenges and overlapping symptoms make timely identification complex, potentially delaying appropriate interventions. Therapeutic challenges arise from the varied responses to interventions among HFpEF patients, necessitating a personalized, multidisciplinary approach to manage these complications effectively. Ongoing research endeavors aim to deepen our understanding and refine strategies for addressing the intricate complications associated with HFpEF, ultimately enhancing patient outcomes and quality of life.
Consultations
Patients with HFpEF typically present to a primary care provider with complaints of exertional dyspnea, activity intolerance, and fatigue. However, the diagnosis of HFpEF may require the expertise of a cardiologist. Once a diagnosis of HFpEF is made, patients require consultation with the cardiac rehabilitation team, cardiac nursing, and a cardiac dietitian. Underlying comorbidities may necessitate consultation with interventional cardiology, electrophysiology, pulmonology-sleep medicine, endocrinology, or a heart failure specialist. While the primary care team can meet most primary palliative care needs, consultation with social workers, case management, or palliative care specialists may become necessary to identify barriers to adequate care and provide patient- and family-specific support. Evidence supports improved quality of life and decreased hospitalizations in patients with heart failure who receive care at a high-volume heart failure center.[95]
Deterrence and Patient Education
All patients with HFpEF should receive counseling and education that emphasizes compliance with dietary and medical therapies; dietary and medical noncompliance are the most common causes of hospital readmission in patients with heart failure.[96] Additionally, improvement in healthcare literacy is associated with a decreased need for emergency care due to heart failure exacerbations.[96] Although single-session educational interventions offer the same benefits as multisession interventions for most patients with heart failure, patients with lower levels of healthcare literacy may benefit from multisession interventions.[97]
Free, printable patient education handout materials are available here:
What is Heart Failure? A discussion of HFrEF, HFmrEF, and HFpEF explaining LVEF and the signs and symptoms of heart failure.
Coping With Heart Failure. A discussion of patient-led lifestyle behaviors to improve overall well-being and strategies to garner assistance.
Heart Failure: How to be Active. A discussion of ways to safely improve physical activity in patients with heart failure.
Heart Failure: Assessing Your Heart. A generalized discussion of diagnostic testing and therapeutic interventions for heart failure.
Heart Failure: Making Changes to Your Diet. A discussion of the adverse effects of fluid overload and excess sodium, including daily sodium goals, how to read food labels, and when to contact a healthcare practitioner.
Heart Failure: Tracking Your Weight. A discussion of the importance of regular weight tracking, including instructions for properly using a weight chart.
Heart Failure: Warning Signs of a Flare-Up. A discussion of the signs and symptoms that may indicate the acute decompensation of heart failure and when to contact a healthcare practitioner.
Taking Medicine to Control Heart Failure. A discussion of strategies to include compliance with heart failure medications, including diuretics, SGLT2 inhibitors, aldosterone blockers, beta blockers, angiotensin receptor neprilysin inhibitors, angiotensin receptor blockers, ACE inhibitors, hydralazine and nitrates, digoxin, sinus node I-f channel blockers, and statins.
Enhancing Healthcare Team Outcomes
The management of HFpEF requires a collaborative effort among healthcare professionals, including physicians, advanced practice providers, nurses, pharmacists, and others, to enhance patient-centered care, improve outcomes, ensure patient safety, and optimize team performance. Given that heart failure represents a common endpoint for various disease processes, including ischemic heart disease secondary to coronary artery disease, addressing the underlying etiologies and risk factors is crucial.
HFpEF is a heterogeneous clinical syndrome with predisposing conditions that involve increasing age, female sex, atrial fibrillation, pulmonary hypertension, obesity, and diabetes. Additionally, HFpEF may result from multiple risk factors, including sleep apnea, chronic obstructive pulmonary disease, iron deficiency, coronary artery disease, atrial fibrillation, and dysrhythmias. The complexity of HFpEF necessitates a multidisciplinary approach, and the exact pathogenic role of each risk factor remains incompletely understood.
Diagnosing HFpEF is challenging due to common clinical manifestations and the overlap with other heart failure subtypes. Diagnostic algorithms, such as HFA-PEFF and H2FPEF, along with additional testing like echocardiography and natriuretic peptide measurement, are employed to confirm the diagnosis. The 2022 AHA/ACC/HFSA Guideline for the Management of Heart Failure provides an evidence-based diagnostic approach.
Therapeutic interventions for HFpEF focus on reducing symptoms, improving quality of life, preventing disease progression, and managing comorbidities. Lifestyle modifications, including exercise training, weight loss, and sodium restriction, are cornerstones of treatment. Antihypertensive therapies, including diuretics, ARNIs, ARBs, and MRAs, are recommended, with a blood pressure goal lower than 130/80 mm Hg. Beta-blockers, sacubitril-valsartan, and sodium-glucose cotransporter 2 inhibitors (SGLT2i) are shown to have beneficial effects. Consultation with sleep medicine is recommended in patients with HFpEF and suspected sleep apnea.
For acute decompensation of HFpEF, a multidisciplinary shock team assessment involving intravenous vasopressors, appropriate ventilation support, and diuresis is crucial. Renal replacement therapy may be considered in patients with poor renal function. However, the early initiation of certain medications, such as ACE inhibitors, ARBs, ARNIs, MRAs, SGLT2 inhibitors, and beta-blockers, lacks substantial evidence for preventing major adverse cardiac events in unstable acute decompensated HFpEF.
The 2022 ACC/AHA Guideline emphasizes palliative and supportive care for all patients with heart failure, including those with HFpEF. Primary palliative care should begin early and address high-quality communication, advance care planning, home and case management assistance, and other needs. The complexity of HFpEF necessitates ongoing research and a comprehensive, team-based approach to optimize patient outcomes.
Media
(Click Image to Enlarge)
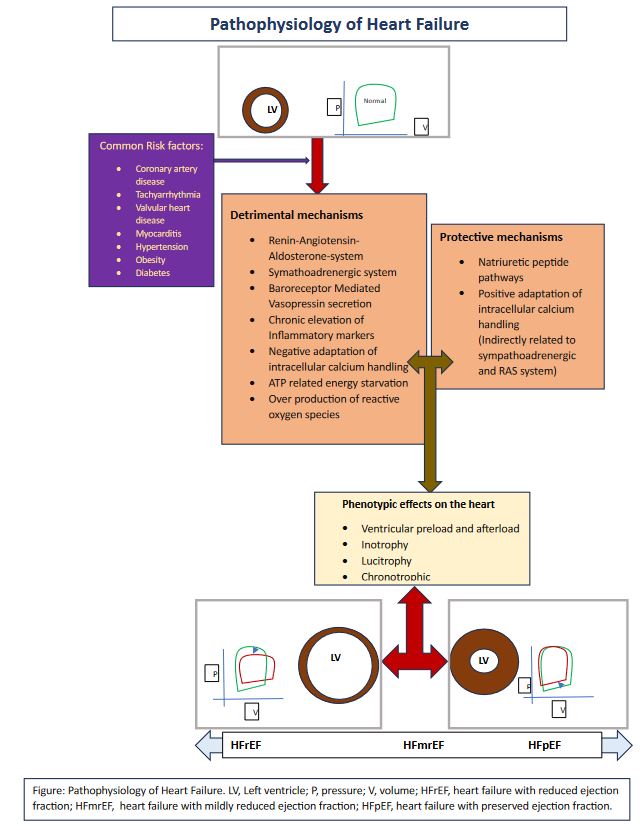
Pathophysiology of Heart Failure
Contributed by MS Golla, MD
(Click Image to Enlarge)
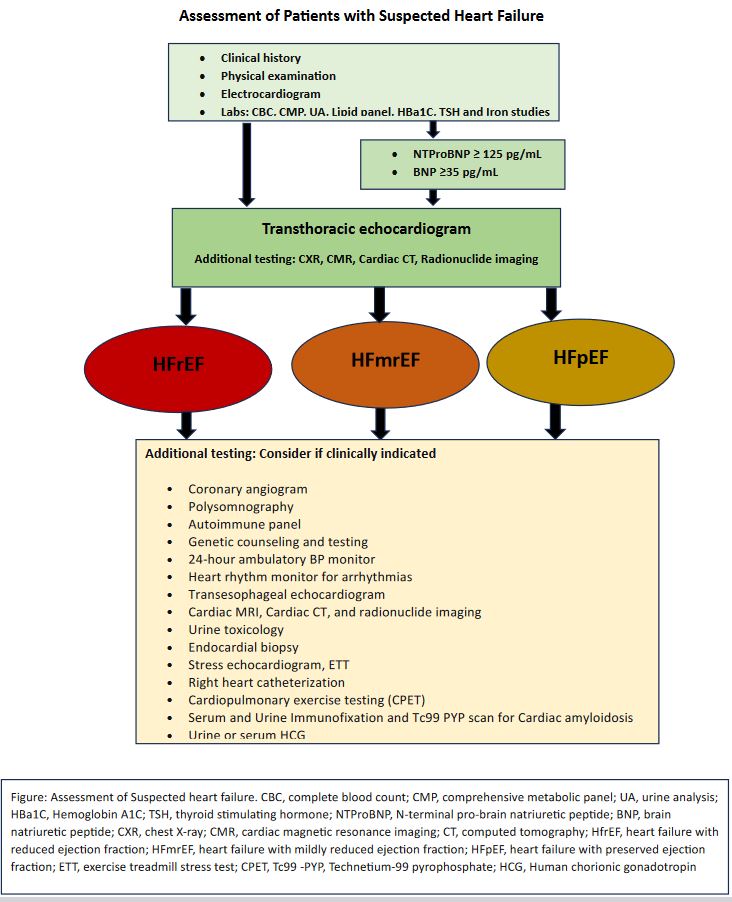
Flowsheet. Assessment of Patients with Suspected Heart Failure
Contributed by MS Golla, MD
References
Heidenreich PA, Bozkurt B, Aguilar D, Allen LA, Byun JJ, Colvin MM, Deswal A, Drazner MH, Dunlay SM, Evers LR, Fang JC, Fedson SE, Fonarow GC, Hayek SS, Hernandez AF, Khazanie P, Kittleson MM, Lee CS, Link MS, Milano CA, Nnacheta LC, Sandhu AT, Stevenson LW, Vardeny O, Vest AR, Yancy CW. 2022 AHA/ACC/HFSA Guideline for the Management of Heart Failure: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Journal of the American College of Cardiology. 2022 May 3:79(17):e263-e421. doi: 10.1016/j.jacc.2021.12.012. Epub 2022 Apr 1 [PubMed PMID: 35379503]
Level 1 (high-level) evidencePfeffer MA, Shah AM, Borlaug BA. Heart Failure With Preserved Ejection Fraction In Perspective. Circulation research. 2019 May 24:124(11):1598-1617. doi: 10.1161/CIRCRESAHA.119.313572. Epub [PubMed PMID: 31120821]
Level 3 (low-level) evidenceZiaeian B, Fonarow GC. Epidemiology and aetiology of heart failure. Nature reviews. Cardiology. 2016 Jun:13(6):368-78. doi: 10.1038/nrcardio.2016.25. Epub 2016 Mar 3 [PubMed PMID: 26935038]
Ammar KA, Jacobsen SJ, Mahoney DW, Kors JA, Redfield MM, Burnett JC Jr, Rodeheffer RJ. Prevalence and prognostic significance of heart failure stages: application of the American College of Cardiology/American Heart Association heart failure staging criteria in the community. Circulation. 2007 Mar 27:115(12):1563-70 [PubMed PMID: 17353436]
Ahmed A, Aronow WS, Fleg JL. Higher New York Heart Association classes and increased mortality and hospitalization in patients with heart failure and preserved left ventricular function. American heart journal. 2006 Feb:151(2):444-50 [PubMed PMID: 16442912]
Reddy YNV, Kaye DM, Handoko ML, van de Bovenkamp AA, Tedford RJ, Keck C, Andersen MJ, Sharma K, Trivedi RK, Carter RE, Obokata M, Verbrugge FH, Redfield MM, Borlaug BA. Diagnosis of Heart Failure With Preserved Ejection Fraction Among Patients With Unexplained Dyspnea. JAMA cardiology. 2022 Sep 1:7(9):891-899. doi: 10.1001/jamacardio.2022.1916. Epub [PubMed PMID: 35830183]
Gazewood JD, Turner PL. Heart Failure with Preserved Ejection Fraction: Diagnosis and Management. American family physician. 2017 Nov 1:96(9):582-588 [PubMed PMID: 29094875]
Rame JE, Ramilo M, Spencer N, Blewett C, Mehta SK, Dries DL, Drazner MH. Development of a depressed left ventricular ejection fraction in patients with left ventricular hypertrophy and a normal ejection fraction. The American journal of cardiology. 2004 Jan 15:93(2):234-7 [PubMed PMID: 14715358]
Tromp J, Shen L, Jhund PS, Anand IS, Carson PE, Desai AS, Granger CB, Komajda M, McKelvie RS, Pfeffer MA, Solomon SD, Køber L, Swedberg K, Zile MR, Pitt B, Lam CSP, McMurray JJV. Age-Related Characteristics and Outcomes of Patients With Heart Failure With Preserved Ejection Fraction. Journal of the American College of Cardiology. 2019 Aug 6:74(5):601-612. doi: 10.1016/j.jacc.2019.05.052. Epub [PubMed PMID: 31370950]
Melenovsky V, Hwang SJ, Redfield MM, Zakeri R, Lin G, Borlaug BA. Left atrial remodeling and function in advanced heart failure with preserved or reduced ejection fraction. Circulation. Heart failure. 2015 Mar:8(2):295-303. doi: 10.1161/CIRCHEARTFAILURE.114.001667. Epub 2015 Jan 15 [PubMed PMID: 25593126]
Zile MR, Baicu CF, Bonnema DD. Diastolic heart failure: definitions and terminology. Progress in cardiovascular diseases. 2005 Mar-Apr:47(5):307-13 [PubMed PMID: 16003645]
Kittleson MM, Panjrath GS, Amancherla K, Davis LL, Deswal A, Dixon DL, Januzzi JL Jr, Yancy CW. 2023 ACC Expert Consensus Decision Pathway on Management of Heart Failure With Preserved Ejection Fraction: A Report of the American College of Cardiology Solution Set Oversight Committee. Journal of the American College of Cardiology. 2023 May 9:81(18):1835-1878. doi: 10.1016/j.jacc.2023.03.393. Epub 2023 Apr 19 [PubMed PMID: 37137593]
Level 3 (low-level) evidenceHe J, Ogden LG, Bazzano LA, Vupputuri S, Loria C, Whelton PK. Risk factors for congestive heart failure in US men and women: NHANES I epidemiologic follow-up study. Archives of internal medicine. 2001 Apr 9:161(7):996-1002 [PubMed PMID: 11295963]
Narita K, Amiya E. Social and environmental risks as contributors to the clinical course of heart failure. Heart failure reviews. 2022 Jul:27(4):1001-1016. doi: 10.1007/s10741-021-10116-7. Epub 2021 May 4 [PubMed PMID: 33945055]
White-Williams C, Rossi LP, Bittner VA, Driscoll A, Durant RW, Granger BB, Graven LJ, Kitko L, Newlin K, Shirey M, American Heart Association Council on Cardiovascular and Stroke Nursing; Council on Clinical Cardiology; and Council on Epidemiology and Prevention. Addressing Social Determinants of Health in the Care of Patients With Heart Failure: A Scientific Statement From the American Heart Association. Circulation. 2020 Jun 2:141(22):e841-e863. doi: 10.1161/CIR.0000000000000767. Epub 2020 Apr 30 [PubMed PMID: 32349541]
Anker SD, Usman MS, Anker MS, Butler J, Böhm M, Abraham WT, Adamo M, Chopra VK, Cicoira M, Cosentino F, Filippatos G, Jankowska EA, Lund LH, Moura B, Mullens W, Pieske B, Ponikowski P, Gonzalez-Juanatey JR, Rakisheva A, Savarese G, Seferovic P, Teerlink JR, Tschöpe C, Volterrani M, von Haehling S, Zhang J, Zhang Y, Bauersachs J, Landmesser U, Zieroth S, Tsioufis K, Bayes-Genis A, Chioncel O, Andreotti F, Agabiti-Rosei E, Merino JL, Metra M, Coats AJS, Rosano GMC. Patient phenotype profiling in heart failure with preserved ejection fraction to guide therapeutic decision making. A scientific statement of the Heart Failure Association, the European Heart Rhythm Association of the European Society of Cardiology, and the European Society of Hypertension. European journal of heart failure. 2023 Jul:25(7):936-955. doi: 10.1002/ejhf.2894. Epub 2023 Jul 17 [PubMed PMID: 37461163]
Savarese G, Becher PM, Lund LH, Seferovic P, Rosano GMC, Coats AJS. Global burden of heart failure: a comprehensive and updated review of epidemiology. Cardiovascular research. 2023 Jan 18:118(17):3272-3287. doi: 10.1093/cvr/cvac013. Epub [PubMed PMID: 35150240]
Lee MP, Glynn RJ, Schneeweiss S, Lin KJ, Patorno E, Barberio J, Levin R, Evers T, Wang SV, Desai RJ. Risk Factors for Heart Failure with Preserved or Reduced Ejection Fraction Among Medicare Beneficiaries: Application of Competing Risks Analysis and Gradient Boosted Model. Clinical epidemiology. 2020:12():607-616. doi: 10.2147/CLEP.S253612. Epub 2020 Jun 15 [PubMed PMID: 32606986]
Reddy YNV, Lewis GD, Shah SJ, Obokata M, Abou-Ezzedine OF, Fudim M, Sun JL, Chakraborty H, McNulty S, LeWinter MM, Mann DL, Stevenson LW, Redfield MM, Borlaug BA. Characterization of the Obese Phenotype of Heart Failure With Preserved Ejection Fraction: A RELAX Trial Ancillary Study. Mayo Clinic proceedings. 2019 Jul:94(7):1199-1209. doi: 10.1016/j.mayocp.2018.11.037. Epub [PubMed PMID: 31272568]
Eaton CB, Pettinger M, Rossouw J, Martin LW, Foraker R, Quddus A, Liu S, Wampler NS, Hank Wu WC, Manson JE, Margolis K, Johnson KC, Allison M, Corbie-Smith G, Rosamond W, Breathett K, Klein L. Risk Factors for Incident Hospitalized Heart Failure With Preserved Versus Reduced Ejection Fraction in a Multiracial Cohort of Postmenopausal Women. Circulation. Heart failure. 2016 Oct:9(10): [PubMed PMID: 27682440]
Chin CWL, Ding ZP, Lam CSP, Ling LH. Paradoxical Low-Gradient Aortic Stenosis: The HFpEF of Aortic Stenosis. Journal of the American College of Cardiology. 2016 May 24:67(20):2447-2448. doi: 10.1016/j.jacc.2016.02.070. Epub [PubMed PMID: 27199070]
Yancy CW, Lopatin M, Stevenson LW, De Marco T, Fonarow GC, ADHERE Scientific Advisory Committee and Investigators. Clinical presentation, management, and in-hospital outcomes of patients admitted with acute decompensated heart failure with preserved systolic function: a report from the Acute Decompensated Heart Failure National Registry (ADHERE) Database. Journal of the American College of Cardiology. 2006 Jan 3:47(1):76-84 [PubMed PMID: 16386668]
Bozkurt B, Ahmad T, Alexander KM, Baker WL, Bosak K, Breathett K, Fonarow GC, Heidenreich P, Ho JE, Hsich E, Ibrahim NE, Jones LM, Khan SS, Khazanie P, Koelling T, Krumholz HM, Khush KK, Lee C, Morris AA, Page RL 2nd, Pandey A, Piano MR, Stehlik J, Stevenson LW, Teerlink JR, Vaduganathan M, Ziaeian B, Writing Committee Members. Heart Failure Epidemiology and Outcomes Statistics: A Report of the Heart Failure Society of America. Journal of cardiac failure. 2023 Oct:29(10):1412-1451. doi: 10.1016/j.cardfail.2023.07.006. Epub 2023 Sep 26 [PubMed PMID: 37797885]
Vasan RS, Enserro DM, Beiser AS, Xanthakis V. Lifetime Risk of Heart Failure Among Participants in the Framingham Study. Journal of the American College of Cardiology. 2022 Jan 25:79(3):250-263. doi: 10.1016/j.jacc.2021.10.043. Epub [PubMed PMID: 35057911]
Pandey A, Omar W, Ayers C, LaMonte M, Klein L, Allen NB, Kuller LH, Greenland P, Eaton CB, Gottdiener JS, Lloyd-Jones DM, Berry JD. Sex and Race Differences in Lifetime Risk of Heart Failure With Preserved Ejection Fraction and Heart Failure With Reduced Ejection Fraction. Circulation. 2018 Apr 24:137(17):1814-1823. doi: 10.1161/CIRCULATIONAHA.117.031622. Epub 2018 Jan 19 [PubMed PMID: 29352072]
Chang PP, Wruck LM, Shahar E, Rossi JS, Loehr LR, Russell SD, Agarwal SK, Konety SH, Rodriguez CJ, Rosamond WD. Trends in Hospitalizations and Survival of Acute Decompensated Heart Failure in Four US Communities (2005-2014): ARIC Study Community Surveillance. Circulation. 2018 Jul 3:138(1):12-24. doi: 10.1161/CIRCULATIONAHA.117.027551. Epub 2018 Mar 8 [PubMed PMID: 29519849]
Tsao CW, Lyass A, Enserro D, Larson MG, Ho JE, Kizer JR, Gottdiener JS, Psaty BM, Vasan RS. Temporal Trends in the Incidence of and Mortality Associated With Heart Failure With Preserved and Reduced Ejection Fraction. JACC. Heart failure. 2018 Aug:6(8):678-685. doi: 10.1016/j.jchf.2018.03.006. Epub 2018 Jul 11 [PubMed PMID: 30007560]
Shiga T, Suzuki A, Haruta S, Mori F, Ota Y, Yagi M, Oka T, Tanaka H, Murasaki S, Yamauchi T, Katoh J, Hattori H, Kikuchi N, Watanabe E, Yamada Y, Haruki S, Kogure T, Suzuki T, Uetsuka Y, Hagiwara N, HIJ-HF II Investigators. Clinical characteristics of hospitalized heart failure patients with preserved, mid-range, and reduced ejection fractions in Japan. ESC heart failure. 2019 Jun:6(3):475-486. doi: 10.1002/ehf2.12418. Epub 2019 Mar 3 [PubMed PMID: 30829002]
Wang N, Hales S, Barin E, Tofler G. Characteristics and outcome for heart failure patients with mid-range ejection fraction. Journal of cardiovascular medicine (Hagerstown, Md.). 2018 Jun:19(6):297-303. doi: 10.2459/JCM.0000000000000653. Epub [PubMed PMID: 29570491]
Chioncel O, Lainscak M, Seferovic PM, Anker SD, Crespo-Leiro MG, Harjola VP, Parissis J, Laroche C, Piepoli MF, Fonseca C, Mebazaa A, Lund L, Ambrosio GA, Coats AJ, Ferrari R, Ruschitzka F, Maggioni AP, Filippatos G. Epidemiology and one-year outcomes in patients with chronic heart failure and preserved, mid-range and reduced ejection fraction: an analysis of the ESC Heart Failure Long-Term Registry. European journal of heart failure. 2017 Dec:19(12):1574-1585. doi: 10.1002/ejhf.813. Epub 2017 Apr 6 [PubMed PMID: 28386917]
Kenchaiah S, Evans JC, Levy D, Wilson PW, Benjamin EJ, Larson MG, Kannel WB, Vasan RS. Obesity and the risk of heart failure. The New England journal of medicine. 2002 Aug 1:347(5):305-13 [PubMed PMID: 12151467]
Kitzman DW, Shah SJ. The HFpEF Obesity Phenotype: The Elephant in the Room. Journal of the American College of Cardiology. 2016 Jul 12:68(2):200-3. doi: 10.1016/j.jacc.2016.05.019. Epub [PubMed PMID: 27386774]
Wong CY, O'Moore-Sullivan T, Leano R, Byrne N, Beller E, Marwick TH. Alterations of left ventricular myocardial characteristics associated with obesity. Circulation. 2004 Nov 9:110(19):3081-7 [PubMed PMID: 15520317]
Russo C, Jin Z, Homma S, Rundek T, Elkind MS, Sacco RL, Di Tullio MR. Effect of obesity and overweight on left ventricular diastolic function: a community-based study in an elderly cohort. Journal of the American College of Cardiology. 2011 Mar 22:57(12):1368-74. doi: 10.1016/j.jacc.2010.10.042. Epub [PubMed PMID: 21414533]
Wohlfahrt P, Redfield MM, Lopez-Jimenez F, Melenovsky V, Kane GC, Rodeheffer RJ, Borlaug BA. Impact of general and central adiposity on ventricular-arterial aging in women and men. JACC. Heart failure. 2014 Oct:2(5):489-99. doi: 10.1016/j.jchf.2014.03.014. Epub 2014 Sep 3 [PubMed PMID: 25194285]
Gorter TM, van Veldhuisen DJ, Bauersachs J, Borlaug BA, Celutkiene J, Coats AJS, Crespo-Leiro MG, Guazzi M, Harjola VP, Heymans S, Hill L, Lainscak M, Lam CSP, Lund LH, Lyon AR, Mebazaa A, Mueller C, Paulus WJ, Pieske B, Piepoli MF, Ruschitzka F, Rutten FH, Seferovic PM, Solomon SD, Shah SJ, Triposkiadis F, Wachter R, Tschöpe C, de Boer RA. Right heart dysfunction and failure in heart failure with preserved ejection fraction: mechanisms and management. Position statement on behalf of the Heart Failure Association of the European Society of Cardiology. European journal of heart failure. 2018 Jan:20(1):16-37. doi: 10.1002/ejhf.1029. Epub 2017 Oct 16 [PubMed PMID: 29044932]
Obokata M, Reddy YNV, Pislaru SV, Melenovsky V, Borlaug BA. Evidence Supporting the Existence of a Distinct Obese Phenotype of Heart Failure With Preserved Ejection Fraction. Circulation. 2017 Jul 4:136(1):6-19. doi: 10.1161/CIRCULATIONAHA.116.026807. Epub 2017 Apr 5 [PubMed PMID: 28381470]
Borlaug BA, Carter RE, Melenovsky V, DeSimone CV, Gaba P, Killu A, Naksuk N, Lerman L, Asirvatham SJ. Percutaneous Pericardial Resection: A Novel Potential Treatment for Heart Failure With Preserved Ejection Fraction. Circulation. Heart failure. 2017 Apr:10(4):e003612. doi: 10.1161/CIRCHEARTFAILURE.116.003612. Epub [PubMed PMID: 28396500]
Borlaug BA, Olson TP, Lam CS, Flood KS, Lerman A, Johnson BD, Redfield MM. Global cardiovascular reserve dysfunction in heart failure with preserved ejection fraction. Journal of the American College of Cardiology. 2010 Sep 7:56(11):845-54. doi: 10.1016/j.jacc.2010.03.077. Epub [PubMed PMID: 20813282]
Haykowsky MJ, Brubaker PH, John JM, Stewart KP, Morgan TM, Kitzman DW. Determinants of exercise intolerance in elderly heart failure patients with preserved ejection fraction. Journal of the American College of Cardiology. 2011 Jul 12:58(3):265-74. doi: 10.1016/j.jacc.2011.02.055. Epub [PubMed PMID: 21737017]
Haykowsky MJ, Kouba EJ, Brubaker PH, Nicklas BJ, Eggebeen J, Kitzman DW. Skeletal muscle composition and its relation to exercise intolerance in older patients with heart failure and preserved ejection fraction. The American journal of cardiology. 2014 Apr 1:113(7):1211-6. doi: 10.1016/j.amjcard.2013.12.031. Epub 2014 Jan 15 [PubMed PMID: 24507172]
Dhakal BP, Malhotra R, Murphy RM, Pappagianopoulos PP, Baggish AL, Weiner RB, Houstis NE, Eisman AS, Hough SS, Lewis GD. Mechanisms of exercise intolerance in heart failure with preserved ejection fraction: the role of abnormal peripheral oxygen extraction. Circulation. Heart failure. 2015 Mar:8(2):286-94. doi: 10.1161/CIRCHEARTFAILURE.114.001825. Epub 2014 Oct 24 [PubMed PMID: 25344549]
Molina AJ, Bharadwaj MS, Van Horn C, Nicklas BJ, Lyles MF, Eggebeen J, Haykowsky MJ, Brubaker PH, Kitzman DW. Skeletal Muscle Mitochondrial Content, Oxidative Capacity, and Mfn2 Expression Are Reduced in Older Patients With Heart Failure and Preserved Ejection Fraction and Are Related to Exercise Intolerance. JACC. Heart failure. 2016 Aug:4(8):636-45. doi: 10.1016/j.jchf.2016.03.011. Epub 2016 May 11 [PubMed PMID: 27179829]
Reddy YNV, Andersen MJ, Obokata M, Koepp KE, Kane GC, Melenovsky V, Olson TP, Borlaug BA. Arterial Stiffening With Exercise in Patients With Heart Failure and Preserved Ejection Fraction. Journal of the American College of Cardiology. 2017 Jul 11:70(2):136-148. doi: 10.1016/j.jacc.2017.05.029. Epub [PubMed PMID: 28683960]
Houstis NE, Eisman AS, Pappagianopoulos PP, Wooster L, Bailey CS, Wagner PD, Lewis GD. Exercise Intolerance in Heart Failure With Preserved Ejection Fraction: Diagnosing and Ranking Its Causes Using Personalized O(2) Pathway Analysis. Circulation. 2018 Jan 9:137(2):148-161. doi: 10.1161/CIRCULATIONAHA.117.029058. Epub 2017 Oct 9 [PubMed PMID: 28993402]
Shah AM, Cikes M, Prasad N, Li G, Getchevski S, Claggett B, Rizkala A, Lukashevich I, O'Meara E, Ryan JJ, Shah SJ, Mullens W, Zile MR, Lam CSP, McMurray JJV, Solomon SD, PARAGON-HF Investigators. Echocardiographic Features of Patients With Heart Failure and Preserved Left Ventricular Ejection Fraction. Journal of the American College of Cardiology. 2019 Dec 10:74(23):2858-2873. doi: 10.1016/j.jacc.2019.09.063. Epub [PubMed PMID: 31806129]
Reddy YNV, Olson TP, Obokata M, Melenovsky V, Borlaug BA. Hemodynamic Correlates and Diagnostic Role of Cardiopulmonary Exercise Testing in Heart Failure With Preserved Ejection Fraction. JACC. Heart failure. 2018 Aug:6(8):665-675. doi: 10.1016/j.jchf.2018.03.003. Epub 2018 May 23 [PubMed PMID: 29803552]
Borbély A, van der Velden J, Papp Z, Bronzwaer JG, Edes I, Stienen GJ, Paulus WJ. Cardiomyocyte stiffness in diastolic heart failure. Circulation. 2005 Feb 15:111(6):774-81 [PubMed PMID: 15699264]
van Heerebeek L, Borbély A, Niessen HW, Bronzwaer JG, van der Velden J, Stienen GJ, Linke WA, Laarman GJ, Paulus WJ. Myocardial structure and function differ in systolic and diastolic heart failure. Circulation. 2006 Apr 25:113(16):1966-73 [PubMed PMID: 16618817]
Zile MR, Baicu CF, Gaasch WH. Diastolic heart failure--abnormalities in active relaxation and passive stiffness of the left ventricle. The New England journal of medicine. 2004 May 6:350(19):1953-9 [PubMed PMID: 15128895]
Zakeri R, Chamberlain AM, Roger VL, Redfield MM. Temporal relationship and prognostic significance of atrial fibrillation in heart failure patients with preserved ejection fraction: a community-based study. Circulation. 2013 Sep 3:128(10):1085-93. doi: 10.1161/CIRCULATIONAHA.113.001475. Epub 2013 Aug 1 [PubMed PMID: 23908348]
Vanderpool RR, Saul M, Nouraie M, Gladwin MT, Simon MA. Association Between Hemodynamic Markers of Pulmonary Hypertension and Outcomes in Heart Failure With Preserved Ejection Fraction. JAMA cardiology. 2018 Apr 1:3(4):298-306. doi: 10.1001/jamacardio.2018.0128. Epub [PubMed PMID: 29541759]
Mohammed SF, Hussain I, AbouEzzeddine OF, Takahama H, Kwon SH, Forfia P, Roger VL, Redfield MM. Right ventricular function in heart failure with preserved ejection fraction: a community-based study. Circulation. 2014 Dec 23:130(25):2310-20. doi: 10.1161/CIRCULATIONAHA.113.008461. Epub 2014 Nov 12 [PubMed PMID: 25391518]
Paulus WJ, Tschöpe C. A novel paradigm for heart failure with preserved ejection fraction: comorbidities drive myocardial dysfunction and remodeling through coronary microvascular endothelial inflammation. Journal of the American College of Cardiology. 2013 Jul 23:62(4):263-71. doi: 10.1016/j.jacc.2013.02.092. Epub 2013 May 15 [PubMed PMID: 23684677]
Franssen C, Chen S, Unger A, Korkmaz HI, De Keulenaer GW, Tschöpe C, Leite-Moreira AF, Musters R, Niessen HW, Linke WA, Paulus WJ, Hamdani N. Myocardial Microvascular Inflammatory Endothelial Activation in Heart Failure With Preserved Ejection Fraction. JACC. Heart failure. 2016 Apr:4(4):312-24. doi: 10.1016/j.jchf.2015.10.007. Epub 2015 Dec 9 [PubMed PMID: 26682792]
Zile MR, Baicu CF, Ikonomidis JS, Stroud RE, Nietert PJ, Bradshaw AD, Slater R, Palmer BM, Van Buren P, Meyer M, Redfield MM, Bull DA, Granzier HL, LeWinter MM. Myocardial stiffness in patients with heart failure and a preserved ejection fraction: contributions of collagen and titin. Circulation. 2015 Apr 7:131(14):1247-59. doi: 10.1161/CIRCULATIONAHA.114.013215. Epub 2015 Jan 30 [PubMed PMID: 25637629]
Bishu K, Hamdani N, Mohammed SF, Kruger M, Ohtani T, Ogut O, Brozovich FV, Burnett JC Jr, Linke WA, Redfield MM. Sildenafil and B-type natriuretic peptide acutely phosphorylate titin and improve diastolic distensibility in vivo. Circulation. 2011 Dec 20:124(25):2882-91. doi: 10.1161/CIRCULATIONAHA.111.048520. Epub 2011 Dec 5 [PubMed PMID: 22144574]
Solomon SD, Rizkala AR, Lefkowitz MP, Shi VC, Gong J, Anavekar N, Anker SD, Arango JL, Arenas JL, Atar D, Ben-Gal T, Boytsov SA, Chen CH, Chopra VK, Cleland J, Comin-Colet J, Duengen HD, Echeverría Correa LE, Filippatos G, Flammer AJ, Galinier M, Godoy A, Goncalvesova E, Janssens S, Katova T, Køber L, Lelonek M, Linssen G, Lund LH, O'Meara E, Merkely B, Milicic D, Oh BH, Perrone SV, Ranjith N, Saito Y, Saraiva JF, Shah S, Seferovic PM, Senni M, Sibulo AS Jr, Sim D, Sweitzer NK, Taurio J, Vinereanu D, Vrtovec B, Widimský J Jr, Yilmaz MB, Zhou J, Zweiker R, Anand IS, Ge J, Lam CSP, Maggioni AP, Martinez F, Packer M, Pfeffer MA, Pieske B, Redfield MM, Rouleau JL, Van Veldhuisen DJ, Zannad F, Zile MR, McMurray JJV. Baseline Characteristics of Patients With Heart Failure and Preserved Ejection Fraction in the PARAGON-HF Trial. Circulation. Heart failure. 2018 Jul:11(7):e004962. doi: 10.1161/CIRCHEARTFAILURE.118.004962. Epub [PubMed PMID: 29980595]
Malik A, Brito D, Vaqar S, Chhabra L. Congestive Heart Failure. StatPearls. 2024 Jan:(): [PubMed PMID: 28613623]
Faxen UL, Venkateshvaran A, Shah SJ, Lam CSP, Svedlund S, Saraste A, Beussink-Nelson L, Lagerstrom Fermer M, Gan LM, Hage C, Lund LH. Generalizability of HFA-PEFF and H(2)FPEF Diagnostic Algorithms and Associations With Heart Failure Indices and Proteomic Biomarkers: Insights From PROMIS-HFpEF. Journal of cardiac failure. 2021 Jul:27(7):756-765. doi: 10.1016/j.cardfail.2021.02.005. Epub 2021 Feb 26 [PubMed PMID: 33647474]
Leggat J, Bidault G, Vidal-Puig A. Lipotoxicity: a driver of heart failure with preserved ejection fraction? Clinical science (London, England : 1979). 2021 Oct 15:135(19):2265-2283. doi: 10.1042/CS20210127. Epub [PubMed PMID: 34643676]
Gerhardt LMS, Kordsmeyer M, Sehner S, Güder G, Störk S, Edelmann F, Wachter R, Pankuweit S, Prettin C, Ertl G, Wanner C, Angermann CE. Prevalence and prognostic impact of chronic kidney disease and anaemia across ACC/AHA precursor and symptomatic heart failure stages. Clinical research in cardiology : official journal of the German Cardiac Society. 2023 Jul:112(7):868-879. doi: 10.1007/s00392-022-02027-w. Epub 2022 Jun 1 [PubMed PMID: 35648270]
Cuthbert JJ, Pellicori P, Rigby A, Pan D, Kazmi S, Shah P, Clark AL. Low serum chloride in patients with chronic heart failure: clinical associations and prognostic significance. European journal of heart failure. 2018 Oct:20(10):1426-1435. doi: 10.1002/ejhf.1247. Epub 2018 Jun 26 [PubMed PMID: 29943886]
Li Y, Li J. Analysis of Risk Factors for Heart Failure with Preserved Ejection Fraction and Observations on Blood Lipid Metabolism. Alternative therapies in health and medicine. 2023 Nov:29(8):396-400 [PubMed PMID: 37632969]
Zhou Q, Yang J, Tang H, Guo Z, Dong W, Wang Y, Meng X, Zhang K, Wang W, Shao C, Hua X, Tang YD. High triglyceride-glucose (TyG) index is associated with poor prognosis of heart failure with preserved ejection fraction. Cardiovascular diabetology. 2023 Sep 29:22(1):263. doi: 10.1186/s12933-023-02001-4. Epub 2023 Sep 29 [PubMed PMID: 37775762]
Salah HM, Pandey A, Soloveva A, Abdelmalek MF, Diehl AM, Moylan CA, Wegermann K, Rao VN, Hernandez AF, Tedford RJ, Parikh KS, Mentz RJ, McGarrah RW, Fudim M. Relationship of Nonalcoholic Fatty Liver Disease and Heart Failure With Preserved Ejection Fraction. JACC. Basic to translational science. 2021 Nov:6(11):918-932. doi: 10.1016/j.jacbts.2021.07.010. Epub 2021 Nov 22 [PubMed PMID: 34869957]
Ponikowski P, van Veldhuisen DJ, Comin-Colet J, Ertl G, Komajda M, Mareev V, McDonagh T, Parkhomenko A, Tavazzi L, Levesque V, Mori C, Roubert B, Filippatos G, Ruschitzka F, Anker SD, CONFIRM-HF Investigators. Beneficial effects of long-term intravenous iron therapy with ferric carboxymaltose in patients with symptomatic heart failure and iron deficiency†. European heart journal. 2015 Mar 14:36(11):657-68. doi: 10.1093/eurheartj/ehu385. Epub 2014 Aug 31 [PubMed PMID: 25176939]
Level 1 (high-level) evidenceDe Luca M, Crisci G, Giardino F, Valente V, Amaranto I, Iacono O, D'Assante R, Giallauria F, Marra AM. Anabolic hormones and heart failure with preserved ejection fraction: looking for Ariadne's thread. Monaldi archives for chest disease = Archivio Monaldi per le malattie del torace. 2021 Aug 3:92(1):. doi: 10.4081/monaldi.2021.1743. Epub 2021 Aug 3 [PubMed PMID: 34351104]
Waddell-Smith KE, Donoghue T, Oates S, Graham A, Crawford J, Stiles MK, Aitken A, Skinner JR. Inpatient detection of cardiac-inherited disease: the impact of improving family history taking. Open heart. 2016:3(1):e000329. doi: 10.1136/openhrt-2015-000329. Epub 2016 Feb 16 [PubMed PMID: 26925241]
Ovchinnikov AG, Ageev FT, Alekhin MN, Belenkov YN, Vasyuk YA, Galyavich AS, Gilyarevskiy SR, Lopatin YM, Mareev VY, Mareev YV, Mitkov VV, Potekhina AV, Prostakova TS, Rybakova MK, Saidova MA, Khadzegova AB, Chernov MY, Yuschuk EN, Boytsov SA. [The role of diastolic transthoracic stress echocardiography with incremental workload in the evaluation of heart failure with preserved ejection fraction: indications, methodology, interpretation. Expert consensus developed under the auspices of the National Medical Research Center of Cardiology, Society of Experts in Heart Failure (SEHF), and Russian Association of Experts in Ultrasound Diagnosis in Medicine (REUDM)]. Kardiologiia. 2021 Jan 19:60(12):48-63. doi: 10.18087/cardio.2020.12.n1219. Epub 2021 Jan 19 [PubMed PMID: 33522468]
Level 3 (low-level) evidencePandey A, Parashar A, Kumbhani D, Agarwal S, Garg J, Kitzman D, Levine B, Drazner M, Berry J. Exercise training in patients with heart failure and preserved ejection fraction: meta-analysis of randomized control trials. Circulation. Heart failure. 2015 Jan:8(1):33-40. doi: 10.1161/CIRCHEARTFAILURE.114.001615. Epub 2014 Nov 16 [PubMed PMID: 25399909]
Level 1 (high-level) evidenceMueller S, Winzer EB, Duvinage A, Gevaert AB, Edelmann F, Haller B, Pieske-Kraigher E, Beckers P, Bobenko A, Hommel J, Van de Heyning CM, Esefeld K, von Korn P, Christle JW, Haykowsky MJ, Linke A, Wisløff U, Adams V, Pieske B, van Craenenbroeck EM, Halle M, OptimEx-Clin Study Group. Effect of High-Intensity Interval Training, Moderate Continuous Training, or Guideline-Based Physical Activity Advice on Peak Oxygen Consumption in Patients With Heart Failure With Preserved Ejection Fraction: A Randomized Clinical Trial. JAMA. 2021 Feb 9:325(6):542-551. doi: 10.1001/jama.2020.26812. Epub [PubMed PMID: 33560320]
Level 1 (high-level) evidenceKitzman DW, Brubaker P, Morgan T, Haykowsky M, Hundley G, Kraus WE, Eggebeen J, Nicklas BJ. Effect of Caloric Restriction or Aerobic Exercise Training on Peak Oxygen Consumption and Quality of Life in Obese Older Patients With Heart Failure With Preserved Ejection Fraction: A Randomized Clinical Trial. JAMA. 2016 Jan 5:315(1):36-46. doi: 10.1001/jama.2015.17346. Epub [PubMed PMID: 26746456]
Level 1 (high-level) evidenceHummel SL, Seymour EM, Brook RD, Sheth SS, Ghosh E, Zhu S, Weder AB, Kovács SJ, Kolias TJ. Low-sodium DASH diet improves diastolic function and ventricular-arterial coupling in hypertensive heart failure with preserved ejection fraction. Circulation. Heart failure. 2013 Nov:6(6):1165-71. doi: 10.1161/CIRCHEARTFAILURE.113.000481. Epub 2013 Aug 28 [PubMed PMID: 23985432]
Faselis C, Arundel C, Patel S, Lam PH, Gottlieb SS, Zile MR, Deedwania P, Filippatos G, Sheriff HM, Zeng Q, Morgan CJ, Wopperer S, Nguyen T, Allman RM, Fonarow GC, Ahmed A. Loop Diuretic Prescription and 30-Day Outcomes in Older Patients With Heart Failure. Journal of the American College of Cardiology. 2020 Aug 11:76(6):669-679. doi: 10.1016/j.jacc.2020.06.022. Epub [PubMed PMID: 32762901]
Cleland JGF, Bunting KV, Flather MD, Altman DG, Holmes J, Coats AJS, Manzano L, McMurray JJV, Ruschitzka F, van Veldhuisen DJ, von Lueder TG, Böhm M, Andersson B, Kjekshus J, Packer M, Rigby AS, Rosano G, Wedel H, Hjalmarson Å, Wikstrand J, Kotecha D, Beta-blockers in Heart Failure Collaborative Group. Beta-blockers for heart failure with reduced, mid-range, and preserved ejection fraction: an individual patient-level analysis of double-blind randomized trials. European heart journal. 2018 Jan 1:39(1):26-35. doi: 10.1093/eurheartj/ehx564. Epub [PubMed PMID: 29040525]
Level 1 (high-level) evidencePitt B, Pfeffer MA, Assmann SF, Boineau R, Anand IS, Claggett B, Clausell N, Desai AS, Diaz R, Fleg JL, Gordeev I, Harty B, Heitner JF, Kenwood CT, Lewis EF, O'Meara E, Probstfield JL, Shaburishvili T, Shah SJ, Solomon SD, Sweitzer NK, Yang S, McKinlay SM, TOPCAT Investigators. Spironolactone for heart failure with preserved ejection fraction. The New England journal of medicine. 2014 Apr 10:370(15):1383-92. doi: 10.1056/NEJMoa1313731. Epub [PubMed PMID: 24716680]
Level 1 (high-level) evidencePfeffer MA, Claggett B, Assmann SF, Boineau R, Anand IS, Clausell N, Desai AS, Diaz R, Fleg JL, Gordeev I, Heitner JF, Lewis EF, O'Meara E, Rouleau JL, Probstfield JL, Shaburishvili T, Shah SJ, Solomon SD, Sweitzer NK, McKinlay SM, Pitt B. Regional variation in patients and outcomes in the Treatment of Preserved Cardiac Function Heart Failure With an Aldosterone Antagonist (TOPCAT) trial. Circulation. 2015 Jan 6:131(1):34-42. doi: 10.1161/CIRCULATIONAHA.114.013255. Epub 2014 Nov 18 [PubMed PMID: 25406305]
McMurray JJV, Jackson AM, Lam CSP, Redfield MM, Anand IS, Ge J, Lefkowitz MP, Maggioni AP, Martinez F, Packer M, Pfeffer MA, Pieske B, Rizkala AR, Sabarwal SV, Shah AM, Shah SJ, Shi VC, van Veldhuisen DJ, Zannad F, Zile MR, Cikes M, Goncalvesova E, Katova T, Kosztin A, Lelonek M, Sweitzer N, Vardeny O, Claggett B, Jhund PS, Solomon SD. Effects of Sacubitril-Valsartan Versus Valsartan in Women Compared With Men With Heart Failure and Preserved Ejection Fraction: Insights From PARAGON-HF. Circulation. 2020 Feb 4:141(5):338-351. doi: 10.1161/CIRCULATIONAHA.119.044491. Epub 2019 Nov 17 [PubMed PMID: 31736337]
Rist A, Sevre K, Wachtell K, Devereux RB, Aurigemma GP, Smiseth OA, Kjeldsen SE, Julius S, Pitt B, Burnier M, Kreutz R, Oparil S, Mancia G, Zannad F. The current best drug treatment for hypertensive heart failure with preserved ejection fraction. European journal of internal medicine. 2024 Feb:120():3-10. doi: 10.1016/j.ejim.2023.10.008. Epub 2023 Oct 19 [PubMed PMID: 37865559]
Solomon SD, McMurray JJV, Claggett B, de Boer RA, DeMets D, Hernandez AF, Inzucchi SE, Kosiborod MN, Lam CSP, Martinez F, Shah SJ, Desai AS, Jhund PS, Belohlavek J, Chiang CE, Borleffs CJW, Comin-Colet J, Dobreanu D, Drozdz J, Fang JC, Alcocer-Gamba MA, Al Habeeb W, Han Y, Cabrera Honorio JW, Janssens SP, Katova T, Kitakaze M, Merkely B, O'Meara E, Saraiva JFK, Tereshchenko SN, Thierer J, Vaduganathan M, Vardeny O, Verma S, Pham VN, Wilderäng U, Zaozerska N, Bachus E, Lindholm D, Petersson M, Langkilde AM, DELIVER Trial Committees and Investigators. Dapagliflozin in Heart Failure with Mildly Reduced or Preserved Ejection Fraction. The New England journal of medicine. 2022 Sep 22:387(12):1089-1098. doi: 10.1056/NEJMoa2206286. Epub 2022 Aug 27 [PubMed PMID: 36027570]
Anker SD, Butler J, Filippatos G, Ferreira JP, Bocchi E, Böhm M, Brunner-La Rocca HP, Choi DJ, Chopra V, Chuquiure-Valenzuela E, Giannetti N, Gomez-Mesa JE, Janssens S, Januzzi JL, Gonzalez-Juanatey JR, Merkely B, Nicholls SJ, Perrone SV, Piña IL, Ponikowski P, Senni M, Sim D, Spinar J, Squire I, Taddei S, Tsutsui H, Verma S, Vinereanu D, Zhang J, Carson P, Lam CSP, Marx N, Zeller C, Sattar N, Jamal W, Schnaidt S, Schnee JM, Brueckmann M, Pocock SJ, Zannad F, Packer M, EMPEROR-Preserved Trial Investigators. Empagliflozin in Heart Failure with a Preserved Ejection Fraction. The New England journal of medicine. 2021 Oct 14:385(16):1451-1461. doi: 10.1056/NEJMoa2107038. Epub 2021 Aug 27 [PubMed PMID: 34449189]
Böhm M, Butler J, Filippatos G, Ferreira JP, Pocock SJ, Abdin A, Mahfoud F, Brueckmann M, Gollop ND, Iwata T, Ponikowski P, Wanner C, Zannad F, Packer M, Anker SD, EMPEROR-Preserved Trial Committees and Investigators. Empagliflozin Improves Outcomes in Patients With Heart Failure and Preserved Ejection Fraction Irrespective of Age. Journal of the American College of Cardiology. 2022 Jul 5:80(1):1-18. doi: 10.1016/j.jacc.2022.04.040. Epub [PubMed PMID: 35772911]
Joglar JA, Chung MK, Armbruster AL, Benjamin EJ, Chyou JY, Cronin EM, Deswal A, Eckhardt LL, Goldberger ZD, Gopinathannair R, Gorenek B, Hess PL, Hlatky M, Hogan G, Ibeh C, Indik JH, Kido K, Kusumoto F, Link MS, Linta KT, Marcus GM, McCarthy PM, Patel N, Patton KK, Perez MV, Piccini JP, Russo AM, Sanders P, Streur MM, Thomas KL, Times S, Tisdale JE, Valente AM, Van Wagoner DR. 2023 ACC/AHA/ACCP/HRS Guideline for the Diagnosis and Management of Atrial Fibrillation: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation. 2024 Jan 2:149(1):e1-e156. doi: 10.1161/CIR.0000000000001193. Epub 2023 Nov 30 [PubMed PMID: 38033089]
Level 1 (high-level) evidenceAlam A, Van Zyl J, Nayyar N, Hall S, Jermyn R. Improvement in Metabolic Co-Morbidities after Implantation of CardioMEMS in Patients with Heart Failure with Preserved Ejection Fraction Phenotype. Journal of clinical medicine. 2021 Sep 22:10(19):. doi: 10.3390/jcm10194308. Epub 2021 Sep 22 [PubMed PMID: 34640323]
Golla MSG, Brown KN, Gupta N. Percutaneous Transluminal Coronary Arteriography. StatPearls. 2024 Jan:(): [PubMed PMID: 30844185]
Datla S, Verberkt CA, Hoye A, Janssen DJA, Johnson MJ. Multi-disciplinary palliative care is effective in people with symptomatic heart failure: A systematic review and narrative synthesis. Palliative medicine. 2019 Sep:33(8):1003-1016. doi: 10.1177/0269216319859148. Epub 2019 Jul 15 [PubMed PMID: 31307276]
Level 1 (high-level) evidenceCasarett D, Fishman J, O'Dwyer PJ, Barg FK, Naylor M, Asch DA. How should we design supportive cancer care? The patient's perspective. Journal of clinical oncology : official journal of the American Society of Clinical Oncology. 2008 Mar 10:26(8):1296-301. doi: 10.1200/JCO.2007.12.8371. Epub [PubMed PMID: 18323553]
Level 3 (low-level) evidenceWaagstein F, Caidahl K, Wallentin I, Bergh CH, Hjalmarson A. Long-term beta-blockade in dilated cardiomyopathy. Effects of short- and long-term metoprolol treatment followed by withdrawal and readministration of metoprolol. Circulation. 1989 Sep:80(3):551-63 [PubMed PMID: 2548768]
Felker GM, Lee KL, Bull DA, Redfield MM, Stevenson LW, Goldsmith SR, LeWinter MM, Deswal A, Rouleau JL, Ofili EO, Anstrom KJ, Hernandez AF, McNulty SE, Velazquez EJ, Kfoury AG, Chen HH, Givertz MM, Semigran MJ, Bart BA, Mascette AM, Braunwald E, O'Connor CM, NHLBI Heart Failure Clinical Research Network. Diuretic strategies in patients with acute decompensated heart failure. The New England journal of medicine. 2011 Mar 3:364(9):797-805. doi: 10.1056/NEJMoa1005419. Epub [PubMed PMID: 21366472]
Level 1 (high-level) evidenceBrisco-Bacik MA, Ter Maaten JM, Houser SR, Vedage NA, Rao V, Ahmad T, Wilson FP, Testani JM. Outcomes Associated With a Strategy of Adjuvant Metolazone or High-Dose Loop Diuretics in Acute Decompensated Heart Failure: A Propensity Analysis. Journal of the American Heart Association. 2018 Sep 18:7(18):e009149. doi: 10.1161/JAHA.118.009149. Epub [PubMed PMID: 30371181]
Mullens W, Dauw J, Martens P, Verbrugge FH, Nijst P, Meekers E, Tartaglia K, Chenot F, Moubayed S, Dierckx R, Blouard P, Troisfontaines P, Derthoo D, Smolders W, Bruckers L, Droogne W, Ter Maaten JM, Damman K, Lassus J, Mebazaa A, Filippatos G, Ruschitzka F, Dupont M, ADVOR Study Group. Acetazolamide in Acute Decompensated Heart Failure with Volume Overload. The New England journal of medicine. 2022 Sep 29:387(13):1185-1195. doi: 10.1056/NEJMoa2203094. Epub 2022 Aug 27 [PubMed PMID: 36027559]
Kitai T, Miyakoshi C, Morimoto T, Yaku H, Murai R, Kaji S, Furukawa Y, Inuzuka Y, Nagao K, Tamaki Y, Yamamoto E, Ozasa N, Tang WHW, Kato T, Kimura T. Mode of Death Among Japanese Adults With Heart Failure With Preserved, Midrange, and Reduced Ejection Fraction. JAMA network open. 2020 May 1:3(5):e204296. doi: 10.1001/jamanetworkopen.2020.4296. Epub 2020 May 1 [PubMed PMID: 32379331]
Jones RC, Francis GS, Lauer MS. Predictors of mortality in patients with heart failure and preserved systolic function in the Digitalis Investigation Group trial. Journal of the American College of Cardiology. 2004 Sep 1:44(5):1025-9 [PubMed PMID: 15337214]
Schjødt I, Johnsen SP, Strömberg A, DeVore AD, Valentin JB, Løgstrup BB. Evidence-Based Process Performance Measures and Clinical Outcomes in Patients With Incident Heart Failure With Reduced Ejection Fraction: A Danish Nationwide Cohort Study. Circulation. Cardiovascular quality and outcomes. 2022 Apr:15(4):e007973. doi: 10.1161/CIRCOUTCOMES.121.007973. Epub 2022 Mar 11 [PubMed PMID: 35272503]
Level 2 (mid-level) evidenceMurray MD, Tu W, Wu J, Morrow D, Smith F, Brater DC. Factors associated with exacerbation of heart failure include treatment adherence and health literacy skills. Clinical pharmacology and therapeutics. 2009 Jun:85(6):651-8. doi: 10.1038/clpt.2009.7. Epub 2009 Mar 4 [PubMed PMID: 19262464]
DeWalt DA, Schillinger D, Ruo B, Bibbins-Domingo K, Baker DW, Holmes GM, Weinberger M, Macabasco-O'Connell A, Broucksou K, Hawk V, Grady KL, Erman B, Sueta CA, Chang PP, Cene CW, Wu JR, Jones CD, Pignone M. Multisite randomized trial of a single-session versus multisession literacy-sensitive self-care intervention for patients with heart failure. Circulation. 2012 Jun 12:125(23):2854-62. doi: 10.1161/CIRCULATIONAHA.111.081745. Epub 2012 May 9 [PubMed PMID: 22572916]
Level 1 (high-level) evidence